


Are we flying blind with optional hospital capacity reporting?
Whether it's responding to Covid-19 or another threat, real-time hospital capacity and occupancy data is crucial.

Hospital capacity data is now limited. Why that could matter...
When the Covid-19 public health emergency (PHE) officially ended, one of my concerns was that this would mean that we’d immediately or eventually lose data that has helped us track the pandemic. For example, during the PHE, the US government required that hospitals report the number of inpatient hospital and ICU beds they had (capacity) and how many of those beds were full (occupancy). This was a major improvement in our ability to track systemic readiness (for any threat) in something close to real-time.
The power of the information that came out of the hospital capacity reporting requirement was apparent to Inside Medicine data analyst Benjy Renton and me—which is why we built out a dashboard to track it. For example, we determined that this information could be used to identify places where demand for care would likely soon exceed supply. We argued that places like this should take some measures to slow down the spread of Covid at key times, for example during the Omicron wave. The actions we had in mind were simple things like limiting indoor dining capacity (say, by 25% at first), and other limits in crowded settings. The idea was that with a lower “contact rate,” an outbreak could be slowed down enough to keep hospitals safe, without grinding society to a screeching halt as we had to do in the spring of 2020. Our model worked beautifully, and it became part of a national plan developed by former members of the Biden Covid-19 transition workgroup.
These days, hospitals are no longer required to report their capacity and occupancy. That is not a good post-PHE change. As a result, currently, around 37% of hospitals are reporting this information on a voluntary basis.
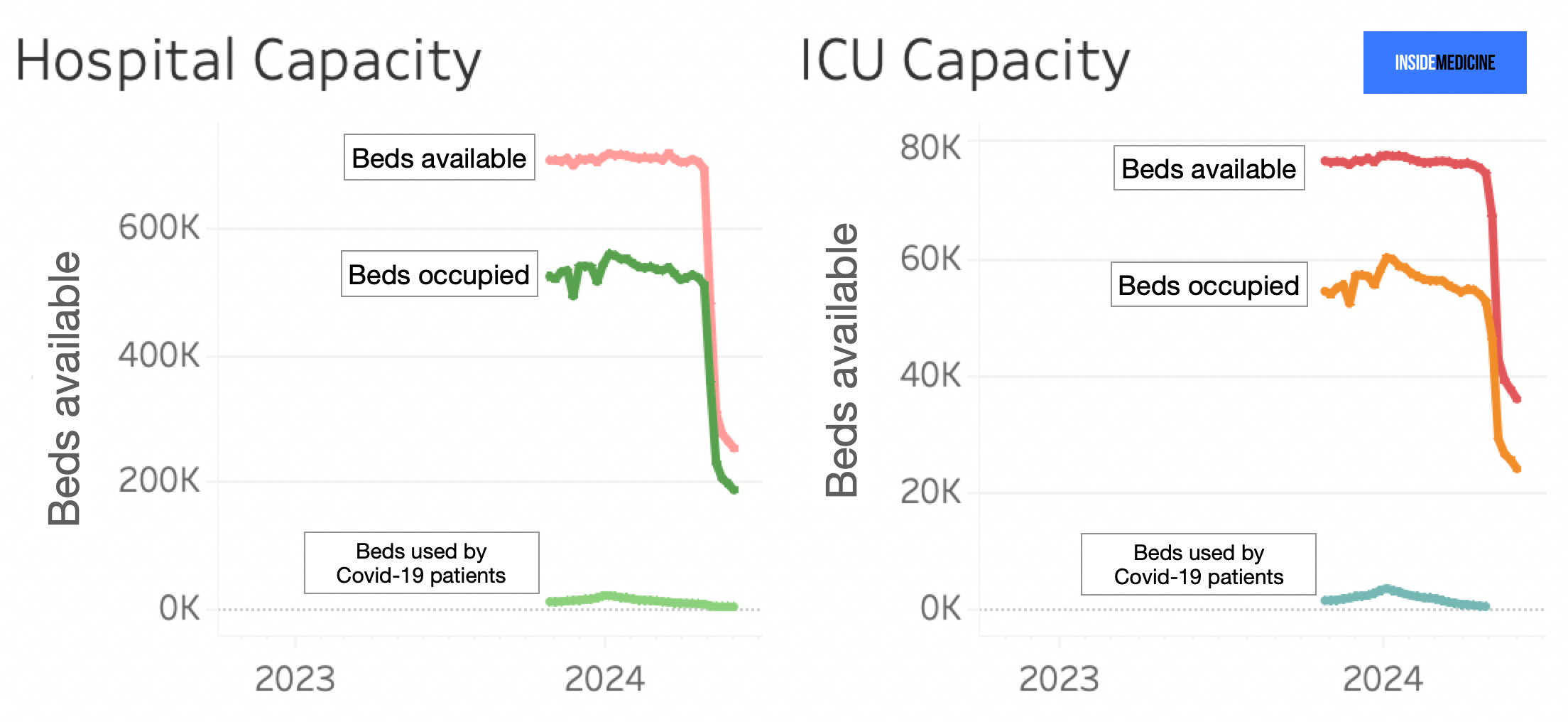
Take a look at our Data Snapshot, taken from our dashboard. You can see when reporting dropped off, once reporting became optional for hospitals.
Are we flying blind here?
It’s hard to say. On one hand, certainly there are areas of the country where the lack of reporting by hospitals could hinder situational awareness among officials and healthcare leaders. On the other, 37% is not a terrible figure from the standpoint of “surveillance.” For example, if you want to know how many trees there are in a forest, you can often count the number in an acre, and just multiply that by how many acres the forest has and get a pretty good idea. So, on a systemic level, it’s possible that the 37% of hospitals voluntarily reporting their capacity and occupancy data are “enough” for us to have a sense of how things stand on a national level. This is the kind of thing that can be studied—and should be. Regardless of the findings, however, from a regional standpoint, there could still easily be dead zones where crucial information is now lacking, due to the now optional reporting. (Like politics, all epidemiology is local.)
Some other observations:
As expected during a typical spring, the percent of inpatient and ICU beds that are occupied right now is lower than in the winter.
Covid accounts for a relatively small percentage of inpatient hospital occupancy. Currently, Covid patients account for around 1% of hospital inpatients, compared to 26% during the Omicron peak. That said, the far lower number today might reflect the fact that universal testing for patients being admitted to the hospital is no longer widespread. (As I’ve long argued, Covid can hospitalize people for reasons that are not quite obvious to medical teams, meaning that the disease might get less credit than it deserves for contributing to a medical emergency requiring hospitalization.)
We can do better….and we actually might!
There is a proposal that would again require hospitals to report on their occupancy and capacity. I strongly favor this. There are many relatively low-value reporting requirements that hospitals must adhere to, lest they get a slap on the wrist from the government. I can think of many such requirements that we could get rid of, with no real consequences. Meanwhile, knowing how ready our nation’s hospitals are for a sudden influx of patients from the next mass casualty incident that emerges—be it a new virus, a Covid-19 variant, or some other disaster—strikes me as critical information. Don’t you agree?
ICYMI: Recent Inside Medicine posts:
First-ever confirmed case of H5N2 influenza in human reported. It was fatal.
My personal experience getting Covid-19, a five-part series:
Part I (premium): My diagnosis, and plans.
Part II: When things got miserable.
Part III (premium): My unusual approach to Paxlovid for my family.
Part IV: Could a smartwatch have prevented my Covid illness?
Part V (premium): Lessons: What I learned (including a time-lapse of 12 daily Covid rapid tests).
Thanks to Benjy Renton for keeping our Inside Medicine Covid and hospital metrics dashboard running!
Dr. Faust, Good post, and informative. Thank you. Recently, it has become my opinion, without any proof, that once a person has endured a Covid infection, the virus has possibly altered their immune system and how their immune system has been coping with infections previously. Their immune system changes - mutates like a virus does - and directs its attention to defending the body against the Covid virus. This change alters the strength of the immune system to defend against heart disease, cancer, lung ailments and other potentially fatal medical ailments. I’ve read opinions that researchers are just considering what the effects of long Covid infections may have for the future health concerns of people with co-morbidities. If this overall observation proves to be true, then the more Covid infections that a person endures, - one, two, three or more - then the worse will be their long term survival chances when one of their other seemingly non-Covid related ailments flares unexpectedly. Medical oncologists have discovered an unexpected flare in progression of Stage 4 cancers in a disproportionate number of their patients who have experienced a Covid infection and when comparing their data, the oncologists wonder if this is related to earlier changes in their patients immune systems due to their Covid infection bouts with the disease. This is too long of an explanation to use when arguing why we should all be extremely careful and be mindful of the presence of the Covid virus everywhere and have our masks at the ready when being inside being in crowded spaces and around other people who may be transmitting a virus that they have mistakenly thought to be gone and forgotten. In my layman’s opinion, Covid is not over.
The past 3-4 weeks my state, Hawaii, has quadrupled (300 to 1200) in weekly case count with a test positivity of 17%. It’s is the only state you have to be in a small enclosed cabin for at least 5 hours to come to, and to leave. Our 2 top economic drivers (people movers) - military and tourism bring close to 1,000,000 arrivals/month in a state with only 1.5M residents.
Are we a canary in a coal mine? An anomaly? What’s your sense of this? Thank you