


Who are the last five people to run CMS before Dr. Oz?
That and other stories in "Five on Friday" for November 22, 2024...



Item 1: Who are the last 5 people to run CMS before Dr. Oz?
Running Medicare and Medicaid is a highly technocratic position. It falls to the Administrator of the Centers for Medicare and Medicaid Services (CMS). CMS is an enormous and complicated operation. CMS ultimately controls $1.5-1.7 trillion per year by supporting programs like Medicare, Medicaid, and the Children's Health Insurance Program (CHIP).
Just take a look at the “org” chart and note how many offices and centers report to the current CMS Administrator Chiquita Brooks-LaSure.

President-elect Donald Trump has proposed Dr. Mehmet Oz as the next person to fill this role. Knowing that, I asked ChatGPT to tell me about the five most recent occupants of the position Dr. Oz might soon fill, if confirmed. Let’s take a look, and then let’s compare the credentials of his predecessors to those of Dr. Oz.
Chiquita Brooks-LaSure (Biden Administration)
Tenure: May 27, 2021 – Present
Prior Experience in Relevant Field:
Director of Coverage Policy at the Department of Health and Human Services (HHS), focusing on ACA implementation.
Staffer on the U.S. House Committee on Ways and Means, working directly on healthcare legislation.
Managing Director at Manatt Health, consulting on CMS policy and ACA-related initiatives.
Experience Level: Extensive experience.
Seema Verma (Trump Administration)
Tenure: March 14, 2017 – January 20, 2021
Prior Experience in Relevant Field:
Consultant for Indiana’s Medicaid expansion and other state-level Medicaid reform programs, including the Healthy Indiana Plan.
Founder and CEO of SVC, Inc., a health policy consulting firm focused on Medicaid policy.
Experience Level: Extensive experience.
Andy Slavitt (Second-term Obama Administration)
Tenure: Acting Administrator, March 18, 2015 – January 20, 2017
Prior Experience in Relevant Field:
Group Executive Vice President at Optum, working on CMS-related healthcare technology and services.
Played a key role in fixing HealthCare.gov during the ACA rollout in direct collaboration with CMS and HHS.
Experience Level: Some experience.
Marilyn Tavenner (First and second-term Obama Administration)
Tenure: December 2, 2011 – March 18, 2015
Prior Experience in Relevant Field:
Secretary of Health and Human Resources for Virginia, overseeing Medicaid and state health programs.
Acting CMS Administrator before formal confirmation.
Hospital administration roles that provided indirect but relevant leadership experience.
Experience Level: Moderate experience.
Donald Berwick (First-term Obama Administration)
Tenure: July 7, 2010 – December 2, 2011
Prior Experience in Relevant Field:
Founder and CEO of the Institute for Healthcare Improvement (IHI), focusing on healthcare quality improvement and cost reduction, closely aligned with CMS priorities.
Advisor to CMS and other national healthcare policy organizations, contributing to CMS quality initiatives.
Experience Level: Extensive experience.
Dr. Mehmet Oz (proposed Second Trump Administration)
Relevant Experience:
Professor of Surgery at Columbia University, focusing on clinical medicine and public health outreach.
Television personality.
No roles directly related to CMS, healthcare policy, or administration.
Experience Level: None.
…Look, I’m not sure what President Trump hopes Dr. Oz will achieve at CMS. But it will certainly be a steep learning curve.
Item 2: Does AI help doctors get the diagnosis?
AI has a lot of potential in medicine (including helping me stay on top of my documentation and simultaneously improve my interactions with patients). A new randomized trial in the Journal of the American Medical Association tested whether physicians were more likely to get the correct diagnosis for a described patient if they were allowed to use AI. The short answer is no. The study volunteers did just as well whether they got to use AI or not. Efficiency was not improved (or hurt) either.
However, a secondary finding has been making headlines, including in the New York Times. When AI was given the same information as the doctors, it outperformed all the doctors—including the ones who could use AI if they wanted to. When doctors used AI, the correct diagnosis was given 76% of the time. But AI alone got the right answer 92% of the time!
Are my colleagues and I already obsolete? No. These clinical cases are highly stylized and they include context clues that make them more like board exam questions than real-life patients. It’s not too surprising that AI can figure out what these “vignettes” are getting at. Real life and board-type questions are pretty different. In fact, many medical students would probably outperform me on Step II of the general medical boards right now, because they are versed in the keywords, hints, and quirks that board exams love. But trust me, that does not mean you want the medical student to be leading your care. (They’ll be ready when they are ready and I’m proud of them!)
So, an interesting set of findings here. The part I was most disappointed with is that AI did not help the doctors. My guess is that it does in real life, but not in highly stylized test environments.
Item 3: What I’m reading: Dr. Paul Offit tried making nice with RFK. Jr.
Getting back to potential Trump appointees, I came across an older essay by vaccine expert, pediatrician, and generally nuanced thinker, Dr. Paul Offit in which he described a phone call he had with RFK Jr. around twenty years ago. At the time, RFK Jr. was a lesser-known quantity and Dr. Offit felt that he could perhaps answer some questions and educate the guy. It did not go well. Dr. Offit says that RFK Jr. not only did not get the message, he also later lied to Joe Rogan about what was said in the conversation. File this one under “no good deed goes unpunished.”
Meanwhile, the American Academy of Pediatrics released a statement of concern regarding RFK Jr.’s nomination to run the US Department of Health and Human Services. The AAP, of course, did not do any name calling or shaming, which is good. It simply stated the facts and its concerns that RFK Jr. seems to not understand issues that are very important to the health of our nation’s children. The primary focus was vaccines. Vaccines, of course, save lives and decrease major illnesses in children. That’s relevant because RFK Jr. has undermined vaccines in his public statements. Per the AAP, “Nearly half of all children in the United States rely on Medicaid or the Children’s Health Insurance Program for their health care, making this process and the policies that flow from HHS leadership critical to children across the country.”
Item 4: Covid-19 antibody updates.
Earlier this year, the FDA authorized a monoclonal antibody against Covid-19 called pemivibart to prevent infections among people with moderate-to-severe immunocompromise. It’s marketed as Pemgarda.
Two papers on pemivibart were published in the New England Journal of Medicine this week. The first is a brief commentary on the use of antibody levels as the main outcome in the studies presented to the FDA. According to the authors, this was the first time this strategy had been used for monoclonal antibody authorization, though similar strategies have been successfully used for vaccines, including for the pediatric Covid-19 vaccines. In that case, lower doses of the vaccines were shown to stimulate antibody levels in kids that resembled those of adults who had received higher doses and had been shown to have much better clinical outcomes (i.e., much less severe disease) than placebo recipients. This is called “immunobridging.” Using this approach to evaluate the effectiveness of monoclonal antibodies in high-risk immunocompromised populations makes some sense, but comes with some concerns for me. The idea of not doing a true clinical trial is it would be unethical to deny the treatment to the placebo group. I’m not sure I buy that in this case (though it is clearly true sometimes). Why not do a study on pemivibart in somewhat lower-risk people? If the antibody prevents infections in them (compared to placebo), it would be reasonable to then use immunobridging for the higher-risk cohort.
The main problem with monoclonal antibodies like pemivibart (and others before it), is that they are highly specific. The second report out in NEJM this week shows that pemivibart may already be out of date, given the newer variants that are circulating. Indeed, new variants tend to render these monoclonal antibodies less useful. That’s why so many have come and gone from the market in just a few years. So, on one hand, the latest data showing that recent Covid variants may make pemivibart less effective would be an argument for immunobridging tests (because it’s faster to get that data). On the other hand, occasional reality checks with clinical data would certainly come in handy. So, I tend to be in the “why not do both” camp.
If any experts here have any additional thoughts on this, please add them in the Comments.
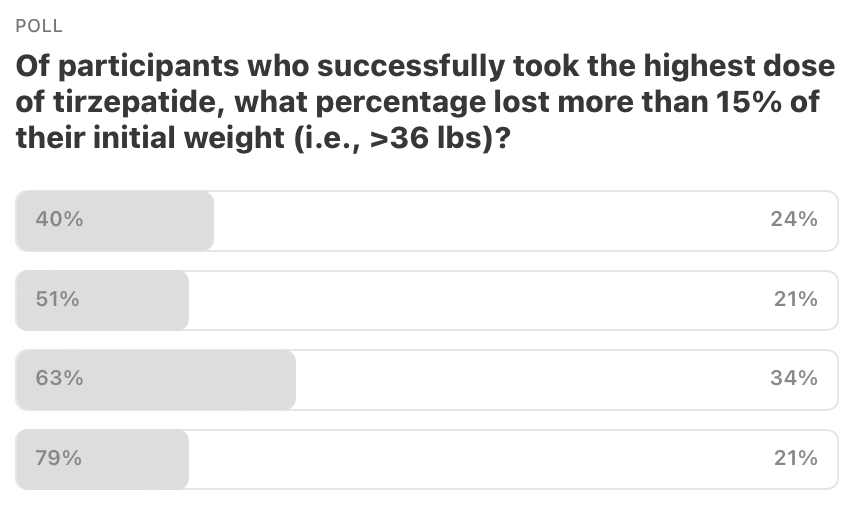
Item 5: Poll of the Week.
Here are the results from the last poll. Thanks for your votes. Most of you underestimated how well tirzepatide works. In fact, 79% of the study volunteers who actually received the drug lost 15% or more of their initial weight. Amazing, isn’t it?
Item 5a: Poll of the Week for this week!
Buckle up. If Dr. Oz takes over CMS, he’ll have a lot of responsibility…
That’s it. Your “Friday Five!” Questions? Comments? Please chime in!

Feedback! Have any ideas for next week’s Poll of the Week? Any great articles you’ve read elsewhere that you want to share with the Inside Medicine community?
Thanks for joining Bluesky. Watch for “starter packs” of docs.
It’s all about P2025. Create chaos and confusion. Trump’s cabinet picks and appointees are photogenic, have extensive experience in front of a TV camera, are typically or have been accused of fraud and sex crimes, and have no relevant experience for their role. To quibble about who’s a better or worse choice by Trump misses the point entirely. It is all about destroying American citizens faith and trust in the government