


Two H5N1 bird flu cases detected California. Where are we headed?
That and other stories in "Five on Friday" for October 4, 2024...



Item 1: Two H5N1 bird flu cases detected California. Where are we headed?
The CDC announced yesterday that two new human cases of H5N1 bird flu have been detected in California. Both patients are thought to have acquired the virus while working in dairies and there appears to be no connection between the two patients. This means that both patients caught the virus directly from cows, rather than via human-to-human spread among potential coworkers. The latter would have been bad news. So far, the 16 knowns cases have been unconnected, with 15 of them occurring in people who work with infected animals. One case (in Missouri) happened in a person without any known animal exposure, raising the possibility of infection from another pathway, like unpasteurized/raw milk.
Where is this all going? A colleague Dr. Nahid Bhadelia (formerly of the White House Coronavirus Taskforce) summarized some of the very same concerns I have in a post on Twitter/X. Even though human-to-human transmission has not yet been detected, are these animal spillover events becoming a new normal? If enough species jumps happen, will human-to-human transmission eventually happen too? Also, if H5N1 is such a bad disease, why have most of the patients had very mild illness (and no deaths)? It’s possible that we have more immunity to H5N1 than we realize. It is also possible that, so far, the disease has affected young and healthy people but that if it infects older and sicker individuals, we could soon see some very severe illness. Lastly, as I wrote yesterday, we could see this virus become more dangerous during the coming cold and flu season if it intermingles with other strains of flu, creating new versions that are either more infectious, causes worse disease, or both.
Item 2: Study: Redlining laws and increased mortality in the 20th century.
A new study in JAMA Internal Medicine found that, compared to people living in the nicest neighborhoods (Home Owners’ Loan Corporation Grade A), people who lived in the least nice neighborhoods (Grade D) had a lower life expectancy, even after controlling for sex, race, and ethnicity.
The cohort of US residents assessed in the study was, on average, around 19 years old in 1940. By the time they reached their 55th birthdays, the mortality differences amounted to 1.44 years of remaining life expectancy. For example, a person who had lived in a Grade A neighborhood might have lived to 80 years old. But a similar person living in Grade D neighborhood in the same era might have lived to 78.
Of course, on the population level, Black people were frequently excluded from the higher grade neighborhoods in the 20th century due to “redlining” laws. That means that this effect was far more common in the Black population—although this study did not measure that, it’s both known and obvious.
There are many reasons why disparities in mortality by race and ethnicity exist. This new paper illuminates just one small and sordid piece of our nation’s history of racism, which, in this case, was literally structural.
Item 3: Opioid replacement medication doses need to be increased.
For many people with opioid use disorder, replacing dangerous drugs like fentanyl with oral medications like buprenorphine or methadone keeps them far safer. These medications treat pain by working on the same receptors as heroin, fentanyl, and other opioids, but without either the high or the life-threatening effects on breathing that come with higher doses. These medications save lives. The problem is that some patients relapse. One reason, researchers believe, is that the standard doses are no longer high enough, due to increasingly strong fentanyl on the illegal market.
Researchers studied this using observational data. In a new paper in JAMA Network Open, the investigators found that patients on doses that exceed the FDA-recommended dose of 16 milligrams ended up in the ER or inpatient units less often (that is, patients on 24 milligram doses, for example, went longer before needing emergency medical services or hospital admission). Also, the higher the dose, the less likely patients were to stop taking buprenorphine. This means that the highest-risk patients who doctors felt needed the greatest quantity of medicine relapsed less than lower-risk patients, an important sub-finding.
Item 4: National Domestic Violence Awareness and Prevention Month.
October is National Domestic Violence Awareness and Prevention Month. This week, President Biden issued a statement summarizing the importance of this issue.
As an emergency doctor, I know that part of my job is to assess patients for signs of domestic violence, which we tend to now call “intimate partner violence.” Non-physician colleague are a major part of our efforts to keep an eye out for this, and it turns out that some fairly brief questionnaires can detect a large number of cases (per a rigorous review of this topic written by two colleagues and friends, Dr. Esther Choo and Dr. Deb Houry.) It’s amazing how powerful asking a few simple questions in the right setting can be.
And even if we don’t detect cases from direct efforts like these screenings/assessments, there are other ways to pick up that something might be wrong, including by noticing conspicuous injury patterns that look different on x-rays compared to typical “innocent” injuries. This is an area where my Brigham and Women’s colleague Dr. Bharti Khurana (and others) have made impressive strides. (Here’s an article I wrote about this in Slate several years ago.)
Physicians and other healthcare professionals play an important role in the detection of intimate partner violence.
But so can anyone.
Per the Biden Administration statement: If you or someone you know is in need of support, immediate and confidential help is available 24/7 through the National Domestic Violence Hotline by visiting thehotline.org, calling 1-800-799-7233 (TTY 1-800-787-3224), or texting “START” to 88788.
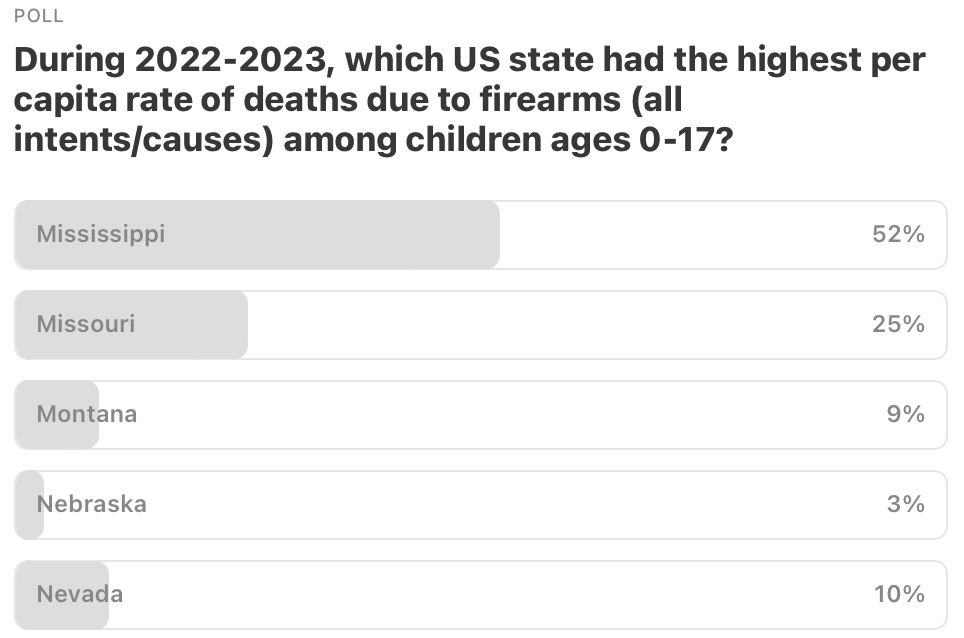
Item 5: Poll of the Week.
Here are the results from the last poll. Thanks for your votes! Mississippi was the correct answer. How’d you all know that?
Item 5a: Poll of the Week for this week!
Medical trivia time. No Google or other resources allowed.
That’s it. Your “Friday Five!” Questions? Comments? Please chime in!

Feedback! Have any ideas for next week’s Poll of the Week? Any great articles you have read elsewhere that you want to share with the Inside Medicine community?