


A new fad: microdosing Ozempic. Why it's unlikely to help most people.

A recent New York Times story described a new fad: “microdosing” GLP-1 anti-obesity drugs like Ozempic, Wegovy, Mounjaro, and Zepbound. I was asked to discuss the topic on CBS News last night, which gave me a chance to look into this topic more deeply. I’d like to share my read on this with you.
The short answer.
There’s no evidence that microdosing—taking very small doses of a GLP-1 in hopes of harnessing the benefits without the side effects—will work for most people. There’s a chance that lower-than-standard doses might help a subset of patients, but if true, it’s likely that the doses would be among the lower doses already tested by the drug companies; that is, lower doses but not truly “micro” doses. Keep in mind, low doses (4-5% of the eventual highest doses now used) failed to show benefits in early trials. However, it’s worth saying that low (but not “micro”) doses could help a select few people who have unusually strong responses to these drugs. Yet, it seems like the microdoses people are taking as part of this fad are a small fraction of even the lowest doses that the drug companies already tested carefully last decade.
To understand why, let’s go Inside Medicine!
The fad.
The Times story described patients using alternative sources for these drugs (telehealth companies) who used compounding pharmacies to prepare much smaller doses than the branded options marketed by the drug companies. All of the blockbuster drugs have standard doses and standardized dose escalation regimens during the “initiation” phase of treatment. The article did not specify what counts as microdosing, but one mentioned dose was 0.05mg (1/5th of the 0.25mg starting dose for Wegovy) which corresponds to 2% of the final 2.4mg milligram dose that patients progress to after 5 months. So, “microdoses” apparently refer to much smaller amounts. We’re talking about 10- or even 100-fold dilutions compared to doses known to work. At some point, the concentration of a compound gets so small that it ceases to be anything, really. For reference, if someone ingested 2% of the lethal dose of cyanide, there’s a good chance that the clinical effect would be nil.
The Times article went on to describe some patient anecdotes indicating that microdosing a GLP-1 had “worked” for them, praising the approach. One patient (who couldn’t tolerate the side effects of the standard doses) concluded that the microdose approach was better than abandoning the drug altogether.
What’s probably happening? Placebo effects.
Hearing that some people believe microdosing GLP-1s has helped them is just not going to cut it. We have to consider the placebo effect. In all of the blinded clinical trials that studied GLP-1s versus placebo, volunteers injecting placebo (not knowing whether they were injecting drug or placebo), lost weight early in the trials. The placebo effect is a well-described phenomenon, but it never ceases to amaze me. The placebo effect is even stronger if you think you’re getting a drug (like a microdose).
Take a look at data from a tirzepatide study in the New England Journal of Medicine (Mounjaro or Zepbound.) People who got placebo lost a bit of weight for a few months. They kept it off during the study, but eventually stopped making progress. Meanwhile, people on low-dose tirzepatide (5mg) lost weight, but not nearly as much as those on 10mg and 15mg, who were still losing weight at the end of the 72-week study.

Many other similar high-quality studies echo this. So, people injecting tiny doses of a GLP-1 are likely subject to the same effects that the placebo recipients in these studies experienced.
Smaller doses have been studied. They act like placebo.
None of that says what would happen if some smaller dose had been used in a clinical trial, such as 1mg of tirzepatide (40% of its standard starting dose and 6.7% of the full dose) or 0.1mg of semaglutide (40% of its standard starting dose and 4.2% of the full dose).
But lower doses like these have been studied. And from those studies, it looks like microdosing—these low doses, and even lower “microdoses”—merely replicates the placebo effects seen in all the clinical trials.
The data from one semaglutide dosing study below shows how much weight volunteers lost, divided by what dose they received, ranging from placebo (far left) to 1.6mg of semaglutide (far right). For context, today, the maximum semaglutide dose for the anti-obesity indication is 2.4mg.

As you can see, those on placebo or the three smallest doses of semaglutide lost between 0.8 kg and 2.0 kg during the 12-week study with no statistically significant differences across these groups. But patients who received 0.8mg (with or without dose escalation) or 1.6mg of semaglutide lost between 3.4 and 4.8 kg (around 4-5% of their initial weight) in that time.
It only took a couple of weeks for the 0.8 and 1.6mg recipients to pull ahead of the low-dose and placebo groups, though the placebo effect tapered off after around 5 weeks. Meanwhile, the 1.6mg recipient group kept losing weight through week 12. So, we can safely say that in this study, very low doses of semaglutide did no better than placebo. And these low doses are not even microdoses; they are likely much stronger. Again, what constitutes microdosing in the anecdotal reports in the Times story was not specified. But the doses are probably a lot smaller than even the low doses that were tested in the study above.
We see this over and over in the trials. The placebo effect works early, and tapers off. Meanwhile, we see dose-response relationships for the drugs themselves (in this case a tirzepatide trial). Somewhat lower doses (5mg) worked for some, but not as well as higher doses. Remember, if you keep lowering the dose, at some point what you’re injecting is no better than placebo. That’s what phase 2 clinical studies are all about: finding doses that are high enough to work, but not so high that their side effects are intolerable or unsafe.
Side effects are lower with lower doses. Thank you, Captain Obvious.
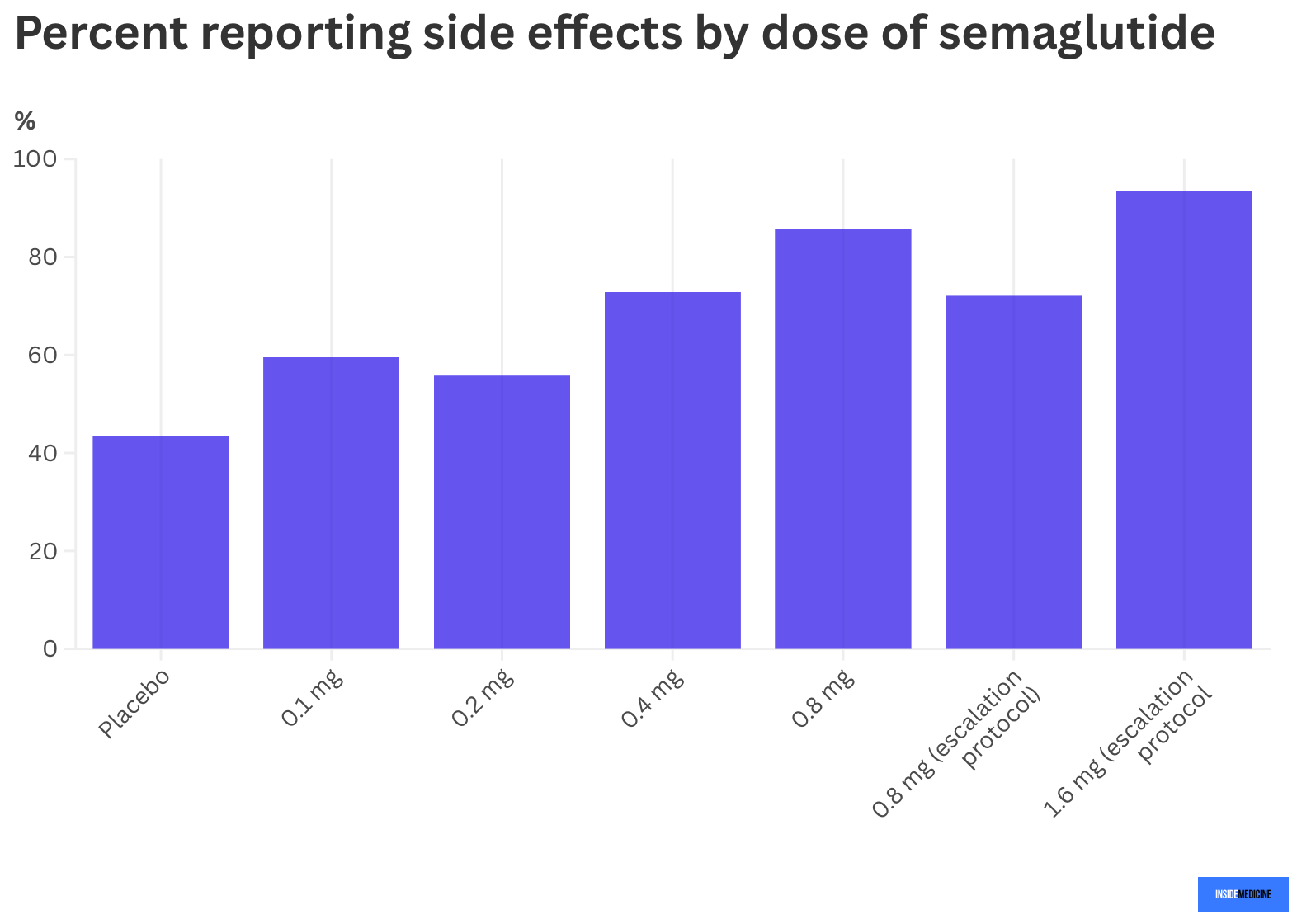
Not surprisingly, in studies, the rate of side effects was lower in those who received smaller doses of the active drugs. The data showed dose-response relationships for both the benefits and the side effects (i.e., the higher the dose, the higher the efficacy and the greater the rate of bothersome side effects). For example, in the tirzepatide study mentioned, 1.7% of placebo recipients reported vomiting compared to 8.3% of those taking 5mg doses, 10.7% of those taking 10mg doses, and 12.2% taking 15mg doses.
In the mentioned semaglutide dosing study, adverse events (side effects) occurred in 43.5% of placebo recipients (the so-called “nocebo” effect wherein people taking placebo still report side effects). From there, generally speaking, the higher the semaglutide dose, the more frequent side effects were. (Note: recipients of 0.8mg doses had lower side effect rates when doses were slowly escalated over weeks, rather than going from nothing to 0.8mg all at once).
What if one-size-fits-all dosing isn’t the only way?
Despite all of this, I’m sympathetic to the idea that one-size-fits-all approach to dosing is not optimal. Indeed, I recently wrote about the fact that clinicians should be open to tweaking dose quantity and scheduling based on individual patients’ responses, rather than just monolithically concluding that a patient having nasty side effects in the dose escalation phase should just give up on the medications entirely. But the notion of microdosing working—that is, getting the benefits without the side effects—is half-baked and untested at best. (At worst, we can say that low doses have been tested and failed. That said, maybe for extremely sensitive responders, a new dosing study is worth doing.)
Could dose changes help some people? Possibly. The way to find out would be to enroll patients who started taking standard GLP-1 dosing regimens but had to stop because the side effects were too burdensome. I’d love to see a dosing trial of patients like this, perhaps looking at smaller initiation doses, or spreading the doses out differently, either by less frequent dosing, or more frequent but lower doses that still get to the same eventual pharmacologic levels. What’s happening now—practitioners prescribing tiny little doses of GLP-1s without any human data to support the practice—is human experimentation that should make us uncomfortable.
What’s the harm?
The main harm of microdosing, as I told CBS News, is the faulty belief that a patient may be taking a drug when, in fact, for all practical purposes, they are not. Imagine planning an overseas trip that requires a Typhoid vaccine. If you received some tiny dose, you might think you’d gotten the needed protected, and proceed to behave accordingly. That could be harmful. GLP-1s don’t just curb obesity, they lower diabetes rates and even mortality in heart disease patients.
Bottom line: Microdosing sounds like a nice idea for a class of drugs with common side effects during the initiation/dose escalation phase of treatment. But, at the moment, the state of the research on microdosing GLP-1s would best be described as fan fiction. The pharmaceutical companies that developed these drugs spent years working out the eventual FDA-approved doses of their active ingredients (semaglutide for Ozempic and Wegovy; tirzepatide for Mounjaro and Zepbound). It’s not likely that lower doses that failed back then (let alone even smaller “microdoses” would suddenly start working for many people now.
Questions? Feedback? Insights? Have you taken these medications? If so, did you have side effects and did they wane over time? Join the conversation!
Can't we learn something about smaller dosage from the weight loss or not of the millions of D2 patients who use Ozempic for glucose control. Max dosage is 2mgs weekly.
Perhaps there should be more studies or conversations regarding this medicine for women in the age group 20-35. I’ve heard of some young women saying the med can negatively affect their mood and sense of daily motivation and when they’ve gone off the med for a break for whatever reason they feel better mood and sense of purpose at work (like studying, doing job, chores, hobbies etc, exercise routine..productivity, connection), so maybe more research in younger adults is needed regarding broader personal daily outcomes and impact around medication management and weekly, monthly dosing. Maybe there should be a questionnaire developed for patient, personal use for discussion points with care providers regarding other kinds of impacts (like being tired or less motivation or less joy, or feeling flatter affect mood, feeling less creativity for example) or other personal impacts of the med effects since it’s a med seemingly used over a longer period of time for different age groups and people at different parts of their personal and work lives.