


We finally have a new monoclonal antibody for Covid-19.
This week's Data Snapshot shows a big, gaping hole.

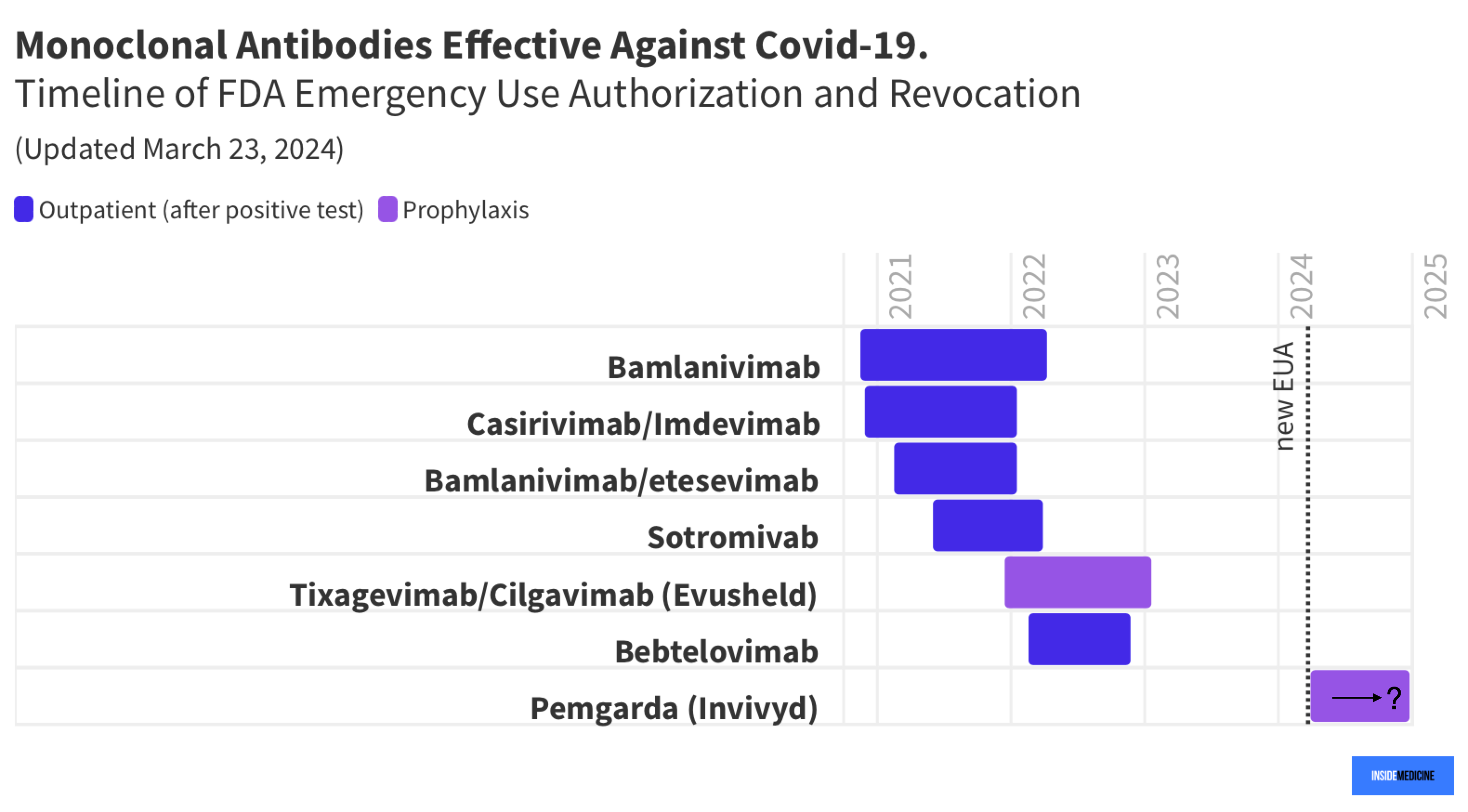
Since January of 2023, we have had no FDA authorized monoclonal antibodies (mABs) for treating or preventing Covid-19. In February of 2023, I wrote about the lack of these mABs, especially pertaining to immunocompromised populations. At that time, the last remaining mAB with FDA authorization for Covid, Evusheld, had just been taken off the market. The loss of Evusheld was a real blow to high-risk individuals. It was the only option ever permitted for use as prophylaxis—that is, to prevent infections among the highest-risk immunocompromised groups. More recently, I argued that perhaps Evusheld should never have been pulled from the market.
We finally have some good news on this front! After a 14-month gap, the FDA has finally authorized a new monoclonal antibody. It’s an injectable called Pemgarda (marketed as “Invivyd”). Like Evusheld, Invivyd is being studied as a prophylactic. Interim data released last week show signs that this new mAB decreases coronavirus infections. If confirmed, this would be a huge win for a key population—one that has been left behind by the winding down of Covid-19 prevention policies since the end of the emergency phase.
Here’s our Data Snapshot, showing the gaping hole in mAB availability from early 2023 until this past week.
Why the gap? The big issue has been that SARS-CoV-2 has been mutating more quickly than might have been anticipated. Now, this is not because of any unexpected change in the virus’s life cycle/mutation rate. Rather, it reflects how many infections there have been, each of which introduces opportunities for mutations to occur (which can render the virus more able to slip past our immunity to it).
Again, look at that 14-month span where immunocompromised people in the US had no pharmacologic option for decreasing infections (other than vaccine boosters, which we more-or-less have been using in this way, which is not ideal):

Not cool. We can and should be doing better.
Why did this long gap in the availability of any mABs occur? The problem is that pharmaceutical companies were spooked by the rate that the virus was mutating and so they stopped producing new ones, after an early rush. The companies understandably did not want to spend hundreds of millions of dollars (or more) developing mABs only to have them rendered insufficiently effective after a matter of months in some cases. All investment, no return.
Many people (I’m one of them) have argued that this would have been a perfect example of an opportunity where public funding could serve as a fiscal safety net, lowering the risk for companies interested in developing much-needed options like Evusheld (and now Invivyd). That problem was compounded by the FDA’s revoking of its authorization for Evusheld based on laboratory data alone, rather than clinical data. All it took for many of these mABs to be taken off the market were a few lab experiments that showed decreased affinity to the latest viral variant. (Increasing the dose and keeping these injectables on the market may, in some instances, have been the better move, in my view. Alas.)
Regardless, Invivyd looks poised to fill a gaping hole in our toolkit against Covid-19, now that the FDA has given it the green light. I’m glad to see this, and hope the final data hold up and that the clinical utility this mAB offers proves to be long-lasting. Some of that will depend on the biology of SARS-CoV-2. But its availability will also depend on the FDA’s decision science.
In addition, the cost of this treatment is not yet known. When it comes to protecting the highest-risk, but relatively small populations, it follows that these drugs may have an eye-popping price tag. Collectively, though, we should be willing to foot that bill. The golden rule applies here.
Questions? Comments? Add them in the Comments section!
Thanks to Benjy Renton for help building the original graphic, which was updated for this post.
If only the golden rule applied here. I recently went to restock my expiring Covid tests and why aren't they subsidized? The average family just can not afford to pay 10$/test. Our "tools" are a slim tool box in my opinion: vaccines that wane quickly, and are reactogenic, Paxlovid--pricey with myriad drug interactions and the requirement of (expensive and possibly less sensitive) rapid tests to identify early infections and successful interaction with the medical system, and no new oral meds in the pipeline--the Japanese oral seems to be languishing and the Gilead oral just got pulled from phase 3 trials. It's disheartening.
Assuming the FDA is led by smart people why are they unable to see what you can see (as well as substackers like Yglesias not trained in science)?