


Smartphone app decreases distracted driving, new trial finds.
Your "Five on Friday" lead story for July 12, 2024...


Special note: I’m devoting this week’s installment of Five on Friday to a group of exceptional new papers which all appeared in JAMA Network Open in just the past few days. It’s unprecedented to devote this feature entirely to papers from a single journal, but I was so impressed with them, that I wanted to share them all with you. (The journal has a new editor-in-chief, who I greatly respect; I’m not sure how many of these papers came on his watch, but I hope this is a sign of more great work to come.)
All of these papers are hot-off-the-press this week. Analyzing them and boiling them down to what you need to know was a lot of work, but is exactly what I want Inside Medicine to be.
So, if you value this and want to support it, please upgrade if you have not already! Thanks! -J

Item 1: Smartphone app decreases distracted driving.
The three major evils behind most fatal auto accidents are drinking while intoxicated, distracted driving, and failure to use a seatbelt. Distracted driving—mostly cell phone use—is a 21st century danger that has not been adequately addressed.
What’s a possible solution to smartphone-based distractions. A smartphone-base app, of course! Indeed, research published in JAMA Network Open points towards potential for progress. Drivers were randomized to a number of different app-based interventions (or control), to see if any of them would decrease the amount of time drivers spent handling their phones. (The apps provided the interventions and the surveillance needed to do the study.)
Some interventions worked, and some did not. The ones that worked combined providing feedback and financial incentives. Interestingly, loss-based financial incentives worked best; that is, drivers were more motivated by the threat of losing a preset amount of money for bad behavior than by being rewarded for good behavior. The amount of financial incentive provided was actually lower than the typical insurance reductions given to drivers with safe records, making this framework feasible as a future model. And that’s important, because once the interventions were discontinued, the improved behavior waned substantially. With over 800,000 motor vehicle crashes caused by distracted driving (and 3,522 deaths) in 2021, the stakes are high here. So the 20% reduction in distracted driving found in drivers who received both feedback and loss-framed financial incentives could save hundreds of lives per year. And maybe larger improvements are possible through enhanced means. Interestingly, the worst quartile of offenders did not show as much improvement as those who were in the second worst quartile, and it could be that these drivers pose an outsized threat. This leaves me wondering whether much higher financial penalties might be necessary to reach the most dangerous segment of distracted drivers.
Item 2: Vaping and secondhand nicotine exposure in kids.
Secondhand smoke from cigarettes has long been understood as a significant health hazard to children. But what about secondhand exposure from vaping?
For starters, outcome severity caused by secondary exposures from vaping are expected to be inherently far milder than those from traditional cigarette smoke. Smoking releases all kinds of hazardous material, inhalation of which can lead to heart disease and cancer. Meanwhile, the junk coming out of vaping is not great, but it’s less dangerous.
A concern around both secondhand cigarette and vape exposure is nicotine, a substance which can harm developing brains. The question is whether secondhand vape exposure is less than that from cigarettes. To answer that, researchers identified kids (ages 3-11) who lived in homes of people who smoke cigarettes or who vape. They then took blood samples and quantified the amount of nicotine exposure in kids living with cigarette or vape users. The findings were published in JAMA Network Open.
Folks, it’s not close.
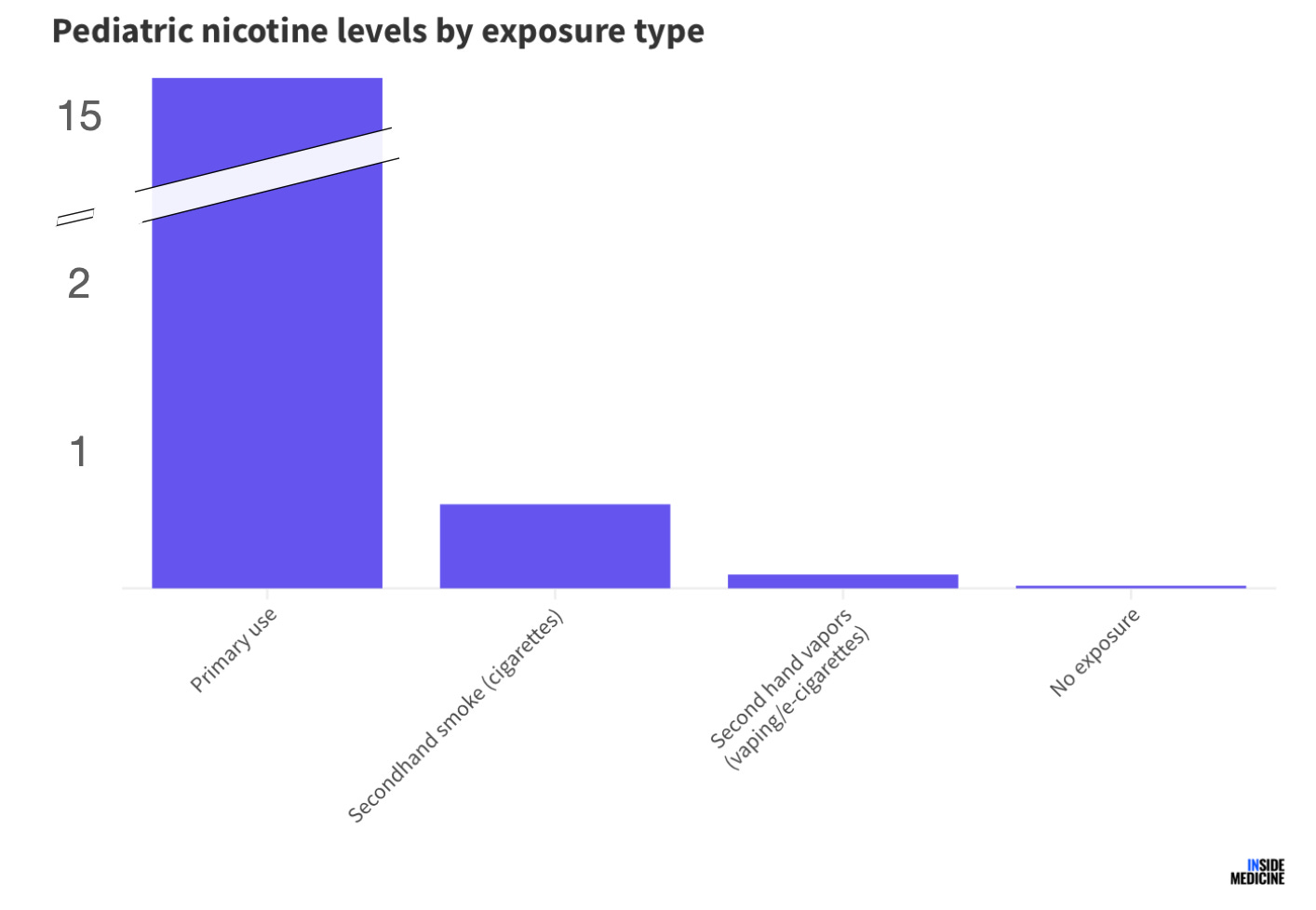
First off, secondhand exposure of any kind is far lower than direct use. (Sadly, two children in the dataset had levels that were high enough to conclude primary use by the kids themselves.) Second, the comparison between secondhand smoke and secondhand vape exposure indicates that kids living with people who vape have 83% lower levels of nicotine in their blood. Of course, no exposure is best.
I continue to grapple with vaping and its “roll” in public health, as we’ve discussed. But in circumstances where it wholesale replaces traditional smoking that would have otherwise occurred, the benefits cannot be ignored.
Item 3: New data adds confidence to RSV vaccine safety during pregnancy.
For decades, an RSV vaccine was elusive. But last year, we finally had vaccines that were safe, effective, and that the CDC recommended (and recently updated) for high-risk groups, including infants and older people. That said, there was a hiccup in one of the trials in which there was a possible increase in the rate of prematurity in infants born to mothers who received the GlaxoSmithKline vaccine during the second trimester of pregnancy. Based on that, the CDC advised RSV vaccination (using Pfizer’s version of a similar vaccine) should occur after week 32 of pregnancy.
Still, there were lingering concerns about whether even that policy might be associated with prematurity. Answer: No. Published this week in JAMA Network Open, researchers in New York assessed their impressive database from last season, and found no increase in premature infants among women who received the Pfizer RSV vaccine. That means that any concern about prematurity related to currently approved RSV vaccines should be minimal (or gone). The result is a vaccine with lower risk than some had feared, but all of the known benefits, including improved infant outcomes among infants born to mothers who received the RSV vaccine during pregnancy.
Item 4: Mental health access via telehealth decreased after the Covid emergency period.
The Covid-19 pandemic did one good thing: it finally moved telehealth from fringe to mainstream. Virtual visits made a huge difference during the emergency period, and for many fields, doing so in perpetuity makes sense.
One such field is mental health. While not all situations are perfectly amenable to virtual visits on Zoom, many are extremely well-suited for them. Unfortunately, access to key mental health services has fallen substantially since the official public health emergency (PHE) ended in 2023. That’s according to a new report in JAMA Network Open. While access to “any” telehealth has not changed since the PHE, access to telehealth for substance use disorders has dropped by 10% (76% during to 66% after), as has telehealth-based psychotherapy (19% absolute decrease) and medication management (a situation in which small tweaks can make a big difference, but the inconvenience of in-person visits may be a barrier).
The telehealth revolution was a piece of unexpected progress brought about by the Covid-19 pandemic. It’s not good to see some of that reversing over time.
Item 5: Poll of the Week.
Here are the results from last week’s poll. Thanks for your votes!

Item 5a: Poll of the Week for this week!
As discussed above, access to mental health services via telehealth has decreased since the height of the Covid-19 pandemic. I’m interested in your views on this topic.
That’s it. Your “Friday Five!”
Feedback! Do you like the “Five on Friday” format? Have any ideas for next week’s Poll of the Week? Any great articles you read elsewhere that you want to share with the Inside Medicine community? Other musings or thoughts?
Please contribute to the Comments!
Love telehealth!
If a clinician remains 100% telehealth (or additionally uses serious air cleaning and mask use in-office), that is a signal they aren't in c0v*d denial - and there's a better chance they won't be dismissive or gaslight-y.