


Scoop: New HHS telework policy leaked.
The document was signed Friday, but only some employees had seen it. Plus four other updates in the Trump war against US public health infrastructure.
Hi everyone! Okay, I have two larger stories (including one HHS-level one scoop and some exclusive insights from our eyes on the ground at the FDA), followed by an update on USAID, and then two shorter hits at the bottom. It’s a lot to catch up on, but these are fascinating and important developments that you’ll want to know about. Let’s get to it. But first…
Just a quick reminder that Inside Medicine is 100% supported by readers who upgrade. Without your support, I can’t do this work. So, your upgrades (and also those “likes” and “shares” that help it reach a broader audience) are what make this all possible. I hope you’ll consider pitching in, if you’re able (and if you can’t upgrade due to financial considerations, just email me and it’s all good). Thank you!
New HHS telework policy leaked. Aligns with Trump administration fiat.

Last Friday, March 14, the Acting Deputy Assistant* Secretary for Human Resources at HHS, Jeffery S. Anoka, signed a new agency-wide telework policy. The leaked document was obtained by Inside Medicine yesterday, but I have not confirmed whether it has been circulated to HHS employees or whether it is officially enacted. It certainly looks like it has been (given the document’s provenance, its verbiage, and the relevant electronic signature), but I have not yet been able to confirm it. That said, on Wednesday I asked numerous people at various agencies (CDC, NIH, and FDA) whether they had seen it, and nobody had (or they did not reply).
UPDATE: After publishing this newsletter this morning, several HHS employees reached out to say that they had been sent the memo, though many others said they still had not.
So, having scrubbed the metadata and all that jazz, I’m just going to post it here:
*Note: Mr. Anoka signed the document with the title “(Acting) Deputy Assistance [sic] Secretary.” It should read “Assistant,” but this administration is allergic to copyeditors.
The upshot is that the Trump administration wants telework to be seen as an exception, not an assumption, which has been the government’s new posture since January 20. The memo states that “[p]articipation in telework programs is not an entitlement but should be based on sound business and performance management principles.” Of course, there is no logic or data suggesting that telework has been anything other than efficient for employees and less expensive for taxpayers, but that’s not the actual point, it turns out.
Because nobody I know at HHS has seen this document (or has seen it but did not reply), and I am inadequately familiar with the prior details of the policy that this new document apparently replaces, I asked ChatGPT to summarize the document and any departures from previous policies.
Here’s what it said (with the caveat that this is what a large language model thinks; if any of this is wrong, I welcome comments and corrections):
Main Points:
Telework is Not an Entitlement
Decisions on telework are based on business needs and performance management.
HHS has broad discretion to set telework levels and exclude certain positions from eligibility.
Stricter Telework Eligibility
Employees must have fully successful performance and no recent discipline to qualify.
Employees on a Performance Improvement Plan (PIP) or with past AWOL issues (5+ days in a year) are ineligible.
Certain jobs may be mandated to work in-office based on mission needs.
Increased Oversight and Compliance
Annual review of telework agreements.
Supervisors must document approvals, modifications, and terminations in writing.
Telework training is required annually for participation.
HR must monitor locality pay and adjust pay rates for remote workers accordingly.
Types of Telework & Changes
Situational/Ad Hoc Telework: Allowed only with prior approval except for emergencies.
Long-Term Telework: Requires HHS approval, mostly for military spouses, disabilities, or approved DETO arrangements.
Mobile Work: For roles requiring travel, such as healthcare workers and inspectors.
Medical Telework: Temporary (3–10 days, max 2 weeks), requiring a doctor’s note.
Return to Office (RTO) Enforcement
Employees may be required to return in person if mission-critical needs arise.
Failure to comply can result in telework suspension or termination.
Employees must report any changes in alternative worksite or risk pay overpayment recoupment.
Impact on Weather & Safety Leave
Telework employees must work during federal office closures unless they take leave.
Only those without telework agreements qualify for weather/safety leave.
Strict Dependent Care Rules
Telework cannot be used as a substitute for dependent care.
Employees must request leave if caregiving interferes with work.
Continuity of Operations Plans & Emergency Operations
Employees designated as mission-critical must report in person during emergencies.
Bottom Line:
HHS is scaling back telework flexibility and reasserting in-person work as the default, aligning with federal return-to-office mandates. Telework is still available but comes with more scrutiny, stricter eligibility, and potential revocation if deemed inconsistent with agency needs.
Musk destruction of USAID likely illegal, judge rules. Reinstatements ordered, while administration changes tactics.
Yesterday, a judge ruled that Elon Musk’s role in the attempted destruction of USAID was unlawful. The order directs the reversal of much of the mayhem that Musk’s DOGE operatives have wrought. According to the New York Times, the decision requires:
“…that agency operations be partially restored, though that reprieve is likely to be temporary. He orderedMr. Musk’s team to reinstate email access to all U.S.A.I.D. employees, including those on paid leave. He also ordered the team to submit a plan for employees to reoccupy a federal office from which they were evicted last month, and he barred Mr. Musk’s team from engaging in any further work “related to the shutdown of U.S.A.I.D.” —The New York Times.
The real question, of course, is what will actually happen.
Indeed, the fate not only of USAID but also of our entire 235-year-old experiment with constitutional democracy and the separation of powers rests on whether judicial orders will be respected by this administration.
So, after the ruling came down, I reached out to Dr. Atul Gawande, who ran global health for USAID during the Biden Administration, and Georgetown Law’s Professor Steve Vladeck. I wanted to know whether they believed the ruling would change much. Their reactions, minutes apart, were so uncanny that (with permission), I simply have to share their texts with you…

It’s like there was a glitch in The Matrix or something.
However, by today, some possibly related action had already been taken, and it was not good news. The AP reported that Secretary of State Marco Rubio has appointed a 20-something DOGE operative, one Jeremy Lewin (no relation #NotAllJeremys), as deputy administrator for policy and programs at USAID and chief operating officer.
This is problematic on two levels. First, giving USAID’s keys to a DOGE operative is a sign that Rubio is now just fine with its continued destruction, despite the fact that he once vocally supported the agency’s programs.
Second, there are signs that the Trump-Musk administration is “going legit” in its attempt to destroy the U.S. federal government. Indeed, the main rationale behind yesterday’s ruling is that Elon Musk and DOGE acted well beyond their permissible duties. In short, putting USAID through the “wood chipper” was not only deplorable but unlawful. But with Marco Rubio on board, similar results could be lawful, though almost equally deplorable. (I qualify with “almost” because if the federal government decides to shut down some programs, it can do that properly; that would at least give stakeholders, employees, and contractors adequate time to reorganize their plans and lives, rather than just pulling the plug without warning on Friday afternoons—and letting people lose their livelihoods instantly, to say nothing of the health and safety of those who benefit from the programs they administer.)
In support of the idea that the administration has concluded that adhering to legal protocol is the better way to destroy or decimate life-saving programs like USAID (and the federal government overall), today the administration provided a court with an update stating that it had followed through on a previous ruling requiring that fulfilled USAID contracts actually be paid. (As a reminder, the Trump administration literally asked the Supreme Court to let it shank on payments for completed work done by USAID contractors, and they only lost 5-4.)
On one hand, it’s good news that the Trump Department of Justice believes it worthwhile to prove to a judge that it is following previous orders. This implies that despite its protestations, the administration actually still believes in the judicial system. On the other hand, it indicates the emergence of a more sophisticated strategy than just firing off likely illegal Executive Orders—an approach that may be slower to unfold, but ultimately more difficult to combat, especially if Congress codifies any of it into its next budget.
An update on the FDA’s in-person work requirement. (Not great, Bob!)
On Monday, I reported on the chaos surrounding the FDA’s attempt to get over 10,000 employees into a campus that was never designed to accommodate such a large workforce.
Since then, the employees we heard from have kept me updated on how things are going (along with input from a couple of new sources). In many ways, things went as expected. In some ways, they were a little better than feared, but largely because rank-and-file employees found ways to make it work.
After a number of conversations, it seems there are at least three partially improvised mitigation measures preventingthe whole thing from falling apart. First, a lot of people used paid time off on Monday and Tuesday to avoid the chaos, so the entire workforce was not actually there. (And some telework actually did happen, although very little; more about that in our next story.) Second, people have been coming to the office as early as 5 a.m. to get parking and avoid long security lines. For example, reports indicate that if you arrive before 6:30 a.m., there is still parking, although some lots and street parking are already filling up by then. Third, once parking runs out, people have been resorting to parking illegally. (As you can see in the photos provided to Inside Medicine by several FDA employees below, the scene looks like a tailgate party. The only troubling things are fire hydrants, lanes, and other access points being blocked.)
A can-do attitude.
“I think everyone is making too much of an effort to make sure it goes smoothly,” one employee told Inside Medicine. “People are still coming in starting at 5 a.m.! Cars are parked everywhere, like on every piece of grass. It’s not sustainable. It looks like a county fairground.” I found it interesting that, on some level, employees were hoping for a dumpster fire, just to prove how inefficient the whole thing is. And yet, an absurdist camaraderie had emerged, described by one employee as “a sense that we won’t be deterred from our public health mission,” even in the face of pointless inefficiency.
One employee said it took half an hour to get out of the parking garage, while another described things as getting a bit better, but still felt “lucky” that it only took him 15 minutes to get out of there on Wednesday.
Not sustainable…which may be the point,
These efforts and inconveniences, however, are likely not sustainable. According to one source, things had already become a bit worse. “There are a lot more cars today, parking decks filled up faster, and parking patterns highlighted the desperation of folks to get a spot on campus.”
On Monday and Tuesday, there was a “sugar high,” one employee said, both “figuratively and literally…people were genuinely excited to see each other and lots of treats being brought in to lighten the mood,” the FDA staffer said.
But by Wednesday, vibes had soured. “Purely anecdotal, but my bus was late so I wasn’t able to prep for an industry meeting like I normally would,” the staffer added. So, by day three, people were already starting to sour on the can-do attitude. This source said he knew someone who had reported almost falling asleep at the wheel today.
While employees praised the operational staff for doing the best it could, there were still delays at security. (One employee expressed feeling bad about having shared a photograph of a long security line on Monday; I assured them that it did not make the security guards look bad, but rather the agency look bad for inadequate provisions.) Still, there was inadequate custodial service, with “no trash pickup, running out of toilet paper and paper towels in the restrooms,” not to mention “slow WiFi and no cell service.” That toilet paper shortage was mentioned by several of our sources.
Nor is any of this likely to be seen by HHS and the Trump administration as particularly problematic, since it seems that the real overall goal here is to reduce the workforce size by making life miserable for federal employees, regardless of the harms this causes Asked whether he felt that “cruelty is the point,” one of the FDA employees agreed. “No doubt. This clearly reduces efficiency, productivity, and morale.”

Two more quick stories…
Here are two other stories I’m following, along with some quick analysis.
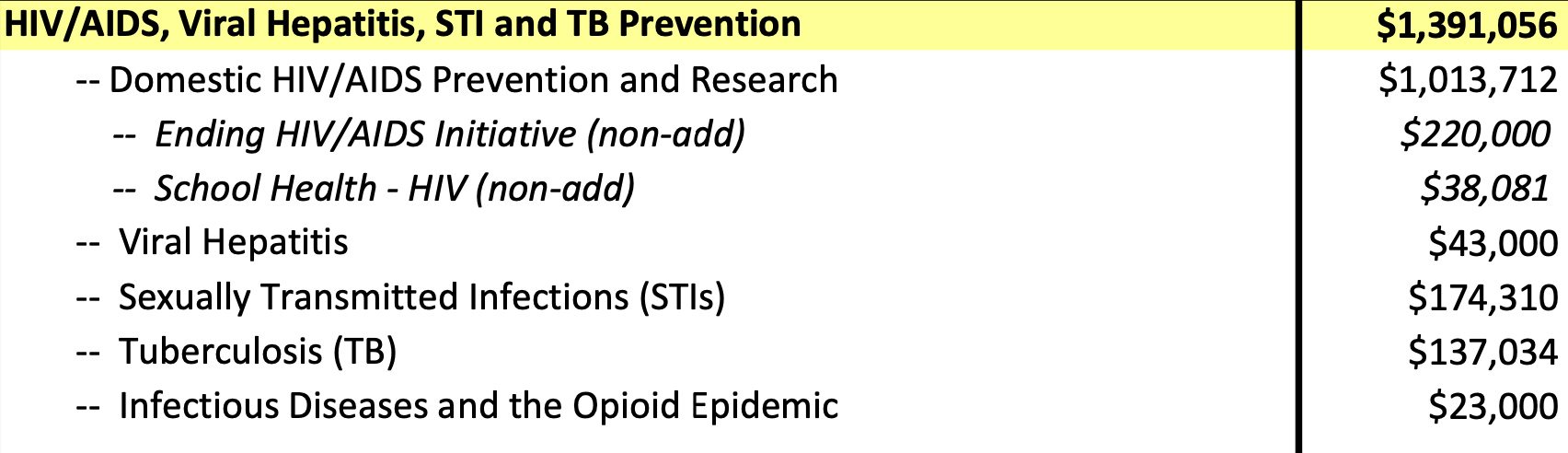
The Wall Street Journal reported that HHS is considering shuttering the CDC’s HIV prevention program. What I want to flag is that under the 2023 Congressional budget, the CDC has to spend $1,391,056,000 on something related to “HIV/AIDS, viral hepatitis, sexually transmitted diseases, and tuberculosis prevention.” That is, unless Congress changes the funding this cycle. So, for now, if the CDC decides to stop its HIV prevention work, it would have to spend the money on something in the above list. They could, of course, find extremely bad uses for that money, but again, at current funding levels, that money would have to be spent. As you can see below, though, most of the budget in this category goes to HIV Prevention.

CDC 2024 spending levels, in thousands of dollars. That said, there are two separate divisions at the CDC focused on HIV. There’s an argument that with lower morbidity and mortality (especially given the incredible progress in prophylaxis), this is an area that could afford a leaner operation. On the other hand, with PEPFAR cuts, this may no longer be the case. Indeed, our retreat from our status as the global leader in the fight against HIV/AIDS is already being felt.
NBC News reported that Johns Hopkins University is laying off 2,000 employees in the wake of USAID cuts. JHU was one of the few institutions I previously highlighted as being at the highest risk for layoffs if NIH grants and other government funding were to disappear. That’s what now seems to be happening.
That’s all for now! If you have information about any of the unfolding stories we are following, please email me or find me on Signal at InsideMedicine.88.
Thanks for reading, sharing, speaking out, and supporting Inside Medicine! Please ask your questions in the comments.
Jeremy, thanks as always. On the telework at HHS, creating chaos and fear is this administration’s super power. For me what stands out is the massive impact of making telework impossible on already marginalized workers. ..i.e. disabled, low income workers who don't own cars, etc. Disabled workers who are the largest marginalized group in the US according to CDC can keep working and contributing to community, support their families, and pay taxes when they are allowed to work from home.
TY so much for your invaluable “inside medicine” reporting. My hair is on fire most days (Jackie Robinson news yesterday)While I am tempted to look away -I can’t. Miraculously I have retained a bit of my sense of humor-like looking at your photo of the parking snarl and likening it to “I am not a robot test” 🤣