


RSV update. Plus new tools in the fight against respiratory illnesses.

Last fall, RSV and influenza season arrived early. (The official cold and flu season starts in October of every year). In October of 2022, we were concerned that increasing rates of RSV-associated hospitalizations so early in the traditional cold and flu season portended bad things for December-March, the typical yearly peak period. Instead, RSV levels topped out in November (albeit at historically high levels for kids), influenza maxed out in December (at fairly typical magnitudes), and both fell off quickly and remained relatively quiet for the winter. For its part, Covid peaked right around the New Year for the 3rd consecutive season, followed by a period of much lower prevalence in the spring, which is pretty typical for a seasonal coronavirus.
October was not as bad as last year.
How’s this year going? Now that we’re into November, we can look at October RSV hospitalization data. We find that last month was neither a replay of the scary October 2022, nor were levels as low as we’d expect based on 2018 and 2019 data, the last pre-Covid Octobers (and the first years for which we have hospitalization data from the CDC). So, basically October of 2023 was somewhere in between for RSV.
You’ll note in the charts below that October of 2023 looks similar to October of 2021-2022. While technically accurate, that does not quite tell the whole story. In the winter of 2020-2021, Covid mitigation knocked RSV and flu out (yes, mitigation worked for lots of viruses). As a result, RSV had an unexpectedly timed resurgence in late summer and early fall of 2021; the end of the 2020-2021 season coincided with a weird RSV surge (generally, there’s almost zero activity at that time of year, making the official seasonal changeover seamless in the data). That meant that when October of 2021 rolled around—the start of the 2021-2022 season—rates were already noticeably high. That all said, October of 2023 did in fact have similar rates compared to 2021. It’s just that the context was just different (i.e., things were overall quite a bit worse in 2021 up to that point). All in all, I’d label October of 2023 as both better and worse than it could have been.
Here are cumulative RSV-associated hospitalizations by season for ages 0-4 and 65 and over in the US since 2018. (You’ll also note that in the two pre-pandemic years, the data stopped in early May. Since the Covid pandemic, the CDC has been tracking everything year round).


The question is whether the traditional RSV peak will occur in the usual timeframe this season. If so, it could be that this year is the first “typical” season for what we might expect going forward for all of our major viruses.
Meanwhile, influenza levels last month were basically nil, unlike October of 2022 when a steady increase was apparent leading to what we now understand was an early peak.
Could this year end up better? We have tools.
RSV hits infants and young children the hardest of any age group. Notice in the graphs above, the Y-axis goes up to 600 hospitalizations per 100,000 children ages 0-4 in the population (top graph) while it barely exceeds 60 hospitalizations per 100,000 adults ages 65 and above. And while I didn’t show it, the rate is 4-6 times higher in infants (up to age 1) compared to young children (ages 1-4). So our youngest are the highest risk for RSV.
The good news is that this season, for the first time, we have new tools to fight RSV. We have newly approved RSV vaccinations for pregnant mothers (shown to protect the eventual infants from getting severe RSV for several months, during crucial vulnerable periods when infant airways are teeny-tiny and thus at risk) and also for adults ages 60 and older. And for babies whose mothers were not vaccinated during pregnancy, we now also have antibody immunizations as options (which are not technically vaccines, but are still effective in decreasing severe disease for that important high-risk period) available for all infants in their first RSV season, and for high-risk infants ages up to 19 months old. (See *update below).
The extent to which these new tools will decrease serious disease and even mortality in infants in our communities overall is unknown—in part because unlike Covid vaccines, I’m not aware of any vaccine tracker that indicates how many pregnant mothers and/or infants received (or are likely to receive) any of these options.
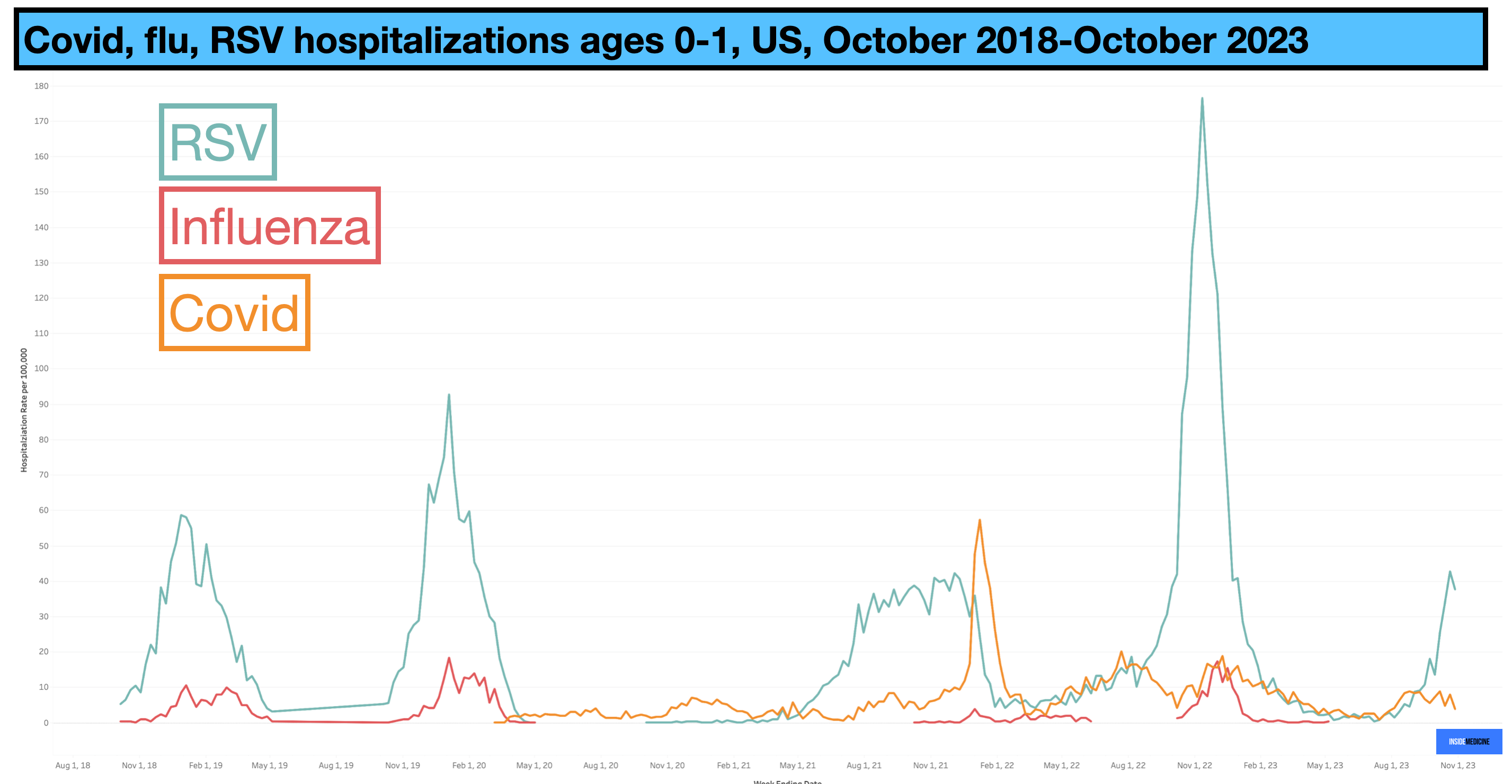
The stakes are relatively high here, though. If you compare Covid, flu, and RSV on the Inside Medicine Respiratory Illness Dashboard in infants up to age 1 (screenshot below), you can see that Covid and RSV hospitalizations have at times dwarfed seasonal influenza hospitalizations. How much of that reflects that we’ve long had annual flu shots for babies (and therefore lower rates of severe disease) is hard to say. But certainly Covid and RSV have caused clinically important disease in infants at times—and now both are, at least in some degree, vaccine-preventable illnesses like flu.
Neither of my kids are eligible for RSV antibodies. But if they were in the right age group, I’d be signing them up. For anyone with children entering their first RSV season (or with high-risk children entering either their first or second season), please ask your pediatrician about the RSV antibody options. (Update: Due to shortages, the CDC has changed its recommendation; currently, rationing requires guidelines to prioritize infants under age 6 months or young children with elevated risks). And if you or your partner is pregnant, ask your physician about getting the RSV vaccine.
It’s nice when we have new tools. It’d be even nicer if we chose to use them.
*Update: A couple of readers pointed out that there is a shortage of Nirsevimab, the long-acting antibody option for infants and young children. As a result, the CDC has changed its guidelines for now. Currently, the RSV immunization is recommended for infants under age 6 months or young children with increased risk for severe disease.
Please give us your thoughts about the RSV vaccine for 60+ given the risk for Gillian Barre.