


Pediatric Covid-19 versus influenza: further thoughts and statistics.
A deeper dive on a comparison that isn’t going away.

This past week, I published an Inside Medicine showing that the Delta and Omicron variants of Covid-19 killed more children in the pediatric population of the United States than seasonal influenza ever does.
This incurred the wrath of some pediatric Covid-19 minimizers. They mistakenly believe that if parents understand Covid-19 to be substantially scarier than flu, we won’t get back to normal things like school soon enough. These crusaders need flu to be worse than Covid or else—they seem to think—they won’t be able to convince parents and teachers to drop their support for testing and mask wearing when needed.
I disagree with that posture. I think acknowledging the reality about Covid-19 in children is what will keep schools both open and safe. The truth is that while Covid-19 is mild in most kids, it is dangerous enough (and so highly contagious) that it has demonstrably caused an enormous burden of death, hospitalization, and downstream consequences in many, many kids. That being the case, it’s worth doing something about.
Actually, the pediatric Covid minimizers and I have something in common: we want schools to be open. But I don’t need Covid-19 to be worse than flu (or vice versa) to get my point across. Even if Covid-19 were in the same ballpark of risk to children as seasonal flu (particularly in terrible flu years), I’d be saying the same thing: control outbreaks by using testing and other forms of surveillance; ask children who are able to mask in high-risk situations at key times; vaccinate children so that when they encounter SARS-CoV-2, it does not cause severe long-term consequences. Keeping Covid at low levels so that our communities are safe requires including children in our mitigation strategies.
That said, since I published my newsletter on this, a lot has happened. First, the article was tweeted by Dr. Ashish Jha, the coordinator of the White House Covid-19 Response Team (i.e. President Biden’s new Covid czar). Then, Bloomberg news published a story that was in effect a summary of my findings in Inside Medicine. This further angered people who have been advancing the talking point that for kids, Covid is just a cold (and no worse than seasonal flu, and maybe even less dangerous). My article even got attacked in the Wall Street Journal.
For the most part, these people repeated old lines that I already addressed (or debunked) in my article. But some made a good point that required a deeper dive.
It was pointed out that the Centers for Disease Control and Prevention (CDC) dataset I used for pediatric Covid-19 included deaths in which Covid contributed to the deaths but was not necessarily the main cause of the deaths (i.e. the underlying cause). Meanwhile, the critics said that the dataset I used for pediatric influenza only included deaths in which flu was the main cause, but not deaths where flu might have contributed. I went back into the datasets and found that this was correct. Now, some critics claimed that this would flip my result, thereby proving the flu is more burdensome on kids than Covid has been. They were wrong. But I did learn some new things and made some revisions. This is why peer review is a good thing. In fact, a couple of colleagues cordially reached out to me (including an official in the federal government) asking me for what researchers call a series of “sensitivity” analyses. That just means asking the same question in several different ways and from different statistical perspectives, to make sure that an overall interpretation is right. So, I did.
Do my main points hold up? Yes.

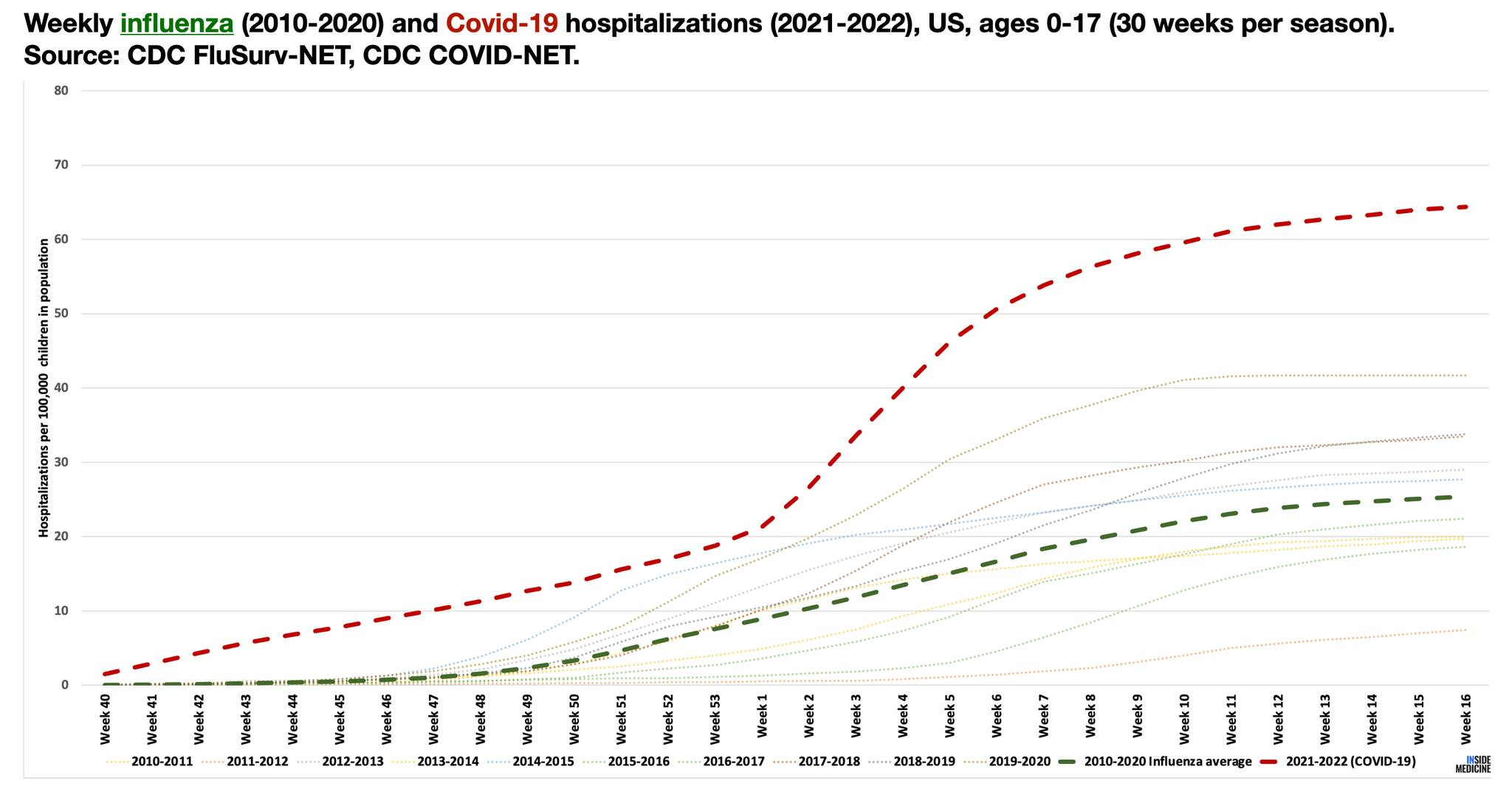
In my original essay, I used data from the yellow line for Covid-19, and data from the red line for influenza. I should have compared data from the green line for Covid-19 to data from the red line for influenza or compared data from the yellow line for Covid-19 to data from the blue line for influenza.
This does make an incremental difference, but the overall findings remain unchanged. To quantify that, and in the interest of transparency, I’m reprinting the relevant paragraphs from my previous article below, but with changes/clarifications/additions in bold.
Covid-19 killed (i.e., appeared on death certificates as either an underlying or contributing cause) 596 (
around 600) children in 2021, which is far more than influenza ever kills in any given year. At the peak of Omicron, 158 (156; two more dead children have been added to the dataset) US children died of Covid-19 in a single month (January 2022). In the 10 years leading up to the Covid-19 pandemic, an average of 150 (120) children died of flu per year—and that was without masking or distancing.
These irrefutable figures, reported by the Centers for Disease Control and Prevention, reveal that last year, pediatric Covid-19 deaths were around 490% (
500%)that of pediatric flu deaths in a typical 21st century season.
Make no mistake: Covid-19 is imparting an unusual burden on children compared to all other respiratory viruses. Since the turn of the century, there have been just 7 instances in which a respiratory virus killed (i.e., appeared on death certificates as an underlying or contributing cause) more than 65 children in a single month in the US. Influenza did it twice: once during the H1N1 pandemic of 2009 (which hit children harder than most realize) and once in March of 2003 (
2009; typo). Covid-19 accounts for each of the other 5 instances, all of which occurred between just August 2021 and February (January; typo) 2022. In fact, of known respiratory viruses, only Covid-19 has ever killed more than 100 US children in a month (underlying cause) in the modern era (for as far back as I can track into the 1990s); it also did so as an underlying or contributing cause) three times during Delta and Omicron alone. Flu did that once (underlying or contributing cause), during the peak of the 2009-2010 H1N1 pandemic.
Based on the original version (i.e the above, minus the bold), I was accused on Twitter of misinformation and lies. I hardly agree. I do think the above clarifies two things: my commitment to showing and checking my work; and that my original analysis was qualitatively correct.
In my earlier piece, I also discussed the differences in statistics reported by two separate centers at the CDC: the National Center for Immunization and Respiratory Diseases (NCIRD) and the National Center for Health Statistics (NCHS). The NCIRD publishes statistics that have been misconstrued by my critics to claim that flu is worse for children than Covid. The NCIRD knows this has been happening and has been working on a response, as I wrote last time.
Well, Inside Medicine and the hullabaloo that followed on Twitter actually caused the CDC’s influenza group at the NCIRD to themselves chime in on Twitter. (I know this is the case because they alerted me about this directly.) Keep in mind that these are the folks who in my view have overestimated pediatric flu burdens over the years (or, at a minimum, have not made it clear what they’re trying to measure). Nevertheless, when it comes to comparing pediatric Covid-19 to influenza, the NCIRD clearly went out of their way to agree with me. I appreciate that.
To review, my critics claim that NCIRD statistics imply that flu typically causes more burden on children than Covid. The NCIRD itself says my critics are wrong and they agree with me.
Of course, the NCIRD could be wrong about their own data! As per the CDC Flu group’s tweet, the NCIRD recently published a paper in a major medical journal that compared its pediatric Covid hospitalization data (COVID-NET) through the fall of 2021 to influenza hospitalization data (FluSurv-NET) from recent years. But the data did not reflect all of Delta and Omicron. Now those numbers are in. So, to check in on the state of things, I ran the latest numbers to see if anything has changed.
As you can see, in the 30 weeks spanning Delta and Omicron, the cumulative number of children hospitalized for Covid (red dashed line) was around 250% that of an average flu season (green dashed line). Remember, during Delta and Omicron, many children and teachers were masking, getting tested, and generally being more careful than during a normal flu season. This likely dampened Covid outbreaks, implying that left unmitigated, the Covid numbers might have been even worse.
In pursuit of fair comparisons, I also compiled the chart below and I invite you to inspect them. If one wishes to cite NCIRD figures on pediatric influenza, then one should also cite NCIRD figures on Covid-19, which rely on similar (albeit not identical) methods. Compare the blue columns. As of October 1st, 2021, NCIRD estimated that 266,597 children had been hospitalized with Covid between February 2020 and the end of September 2021 (or around 160,000 hospitalizations per year). That’s 460% (160,000/34,698) the NCIRD’s average estimate on annual pediatric flu.

If the NCIRD estimates are no longer to your liking, you could compare FluSurv-NET and COVID-NET (yellow columns). Again, while not identical, the surveillance methods of FluSurv-NET and COVID-NET are similar and cover similar regions of the United States. We can see that during the worst 30-week stretch spanning Delta and Omicron, Covid hospitalizations were around 250% (46,606/18,632) that of an average flu season.
You may have noticed that I haven’t discussed infection fatality rates—that is, what percent of children infected die of Covid or flu. That’s because the number of infections is just too hard to know for both diseases. The CDC believes (and I agree) that we fail to detect many cases of flu each year. They also think the same thing is happening with Covid. If we were able to detect every case, we would calculate lower fatality rates for each disease, because we miss a higher proportion of cases (i.e. the mild ones) than deaths. I tend to think Covid is deadlier on a per infection basis than a typical flu, but the data here don’t explicitly prove that.
If we are intent on comparing flu and Covid, we need to ask the right overall question. The most relevant question is not, “would I rather my child contract the flu or Covid?” The better question is, “would I rather have my child encounter a flu outbreak or a Covid outbreak?” The second question encompasses both the number of bad outcomes and the overall number of infections. Covid is clearly more contagious than flu. Even if flu has a higher kill rate than Covid per infection (which, again, I doubt), the “mortality product” (that is, the number of infections in a given period multiplied by the percent of infections that are fatal) is likely far higher for Covid.
On a population level, Covid’s contagiousness combined with its rate of severe outcomes clearly towers over flu—even in children.
If we are discussing “what to do” about an outbreak, population-level statistics are important. Oftentimes, the population fatality rate (i.e. the percent of the entire population that dies from a disease, not just the percent of the infected people that die) or the population hospitalization rate is what matters. (That’s what FluSurv-NET and Covid-NET measure, as it happens.)
Consider two hypothetical diseases. One has a fatality rate of 50% but only spreads via cannibalism. Very few people would die from this disease, as there are very few cannibals. The population fatality rate would be small, because almost nobody would ever catch it. Meanwhile, the second disease is an airborne pathogen with a kill rate of 0.5% (100-times less deadly). It stands to kill millions, as it easily moves through communities. The population fatality rate would be higher, even though the fatality rate per infection of the supposedly milder airborne disease would be lower than the one spread by cannibalism.
There are more ways to look at the pediatric flu and Covid question. We could look at individual states. We could look at different age groups. We could compare Covid to a different disease. Some of these comparisons would make Covid look even worse, and some would make it look better. That’s fine. In public health, we don’t parlay relatively good news about one demographic in order to downplay the risks to another. Instead, we identify the most vulnerable people, and do what we can to protect them. Fortunately for us, we can keep kids safe from Covid-19 without draconian measures like cancelling school for months on end. But twisting data to match an agenda (downplaying the importance of vaccination, keeping kids in school every day, at all costs, with not even an attempt to protect them and their communities from Covid) isn’t the way to go.
❓💡🗣️ What are your questions? Comments? Join the conversation below!
Follow me on Twitter, Instagram, and on Facebook and help me share accurate frontline medical information!
📬 Subscribe to Inside Medicine here and get updates from the frontline at least twice per week.
Acknowledgements: I wish to thank the staff at the National Center for Immunization and Respiratory Diseases at the CDC. We may not 100% agree on every last point, but we share the goal of educating the public in order to reduce vaccine-preventable illnesses, of which Covid and flu are both important examples. Benjy Renton for data analysis.