

New research: Razor thin margins at best on prostate cancer screening benefits.
New research: Razor thin margins at best on prostate cancer screening benefits.

Prostate cancer screening should work better than it does. By measuring prostate specific antigen (PSA) levels in the blood, doctors should be able to detect prostate cancers before symptoms appear and get them treated before they become dangerous or deadly. That is the cornerstone notion of prostate cancer screening.
For reasons that I can’t entirely understand, PSA testing just does not save many lives, if any. No less august a body than the United States Preventive Services Taskforce (USPST) states that men ages 55-69 should consider PSA testing, while weighing the harms and benefits with their doctors. The USPST recommends against PSA testing for men ages 70 and up. Hardly a ringing endorsement. The CDC says no different.
This all surprises a lot of people. I think the messaging in the medical and public health community has often been different from this—a bit too rah-rah in light of the science.
Take a look at new data, published in the Journal of the American Medical Association over the weekend. In the United Kingdom, researchers randomized men to either get an invitation to do prostate cancer screening or not. Then, they followed outcomes for 15 years. If prostate cancer screening made a difference, the mortality curves should have daylight between them. They basically didn’t.
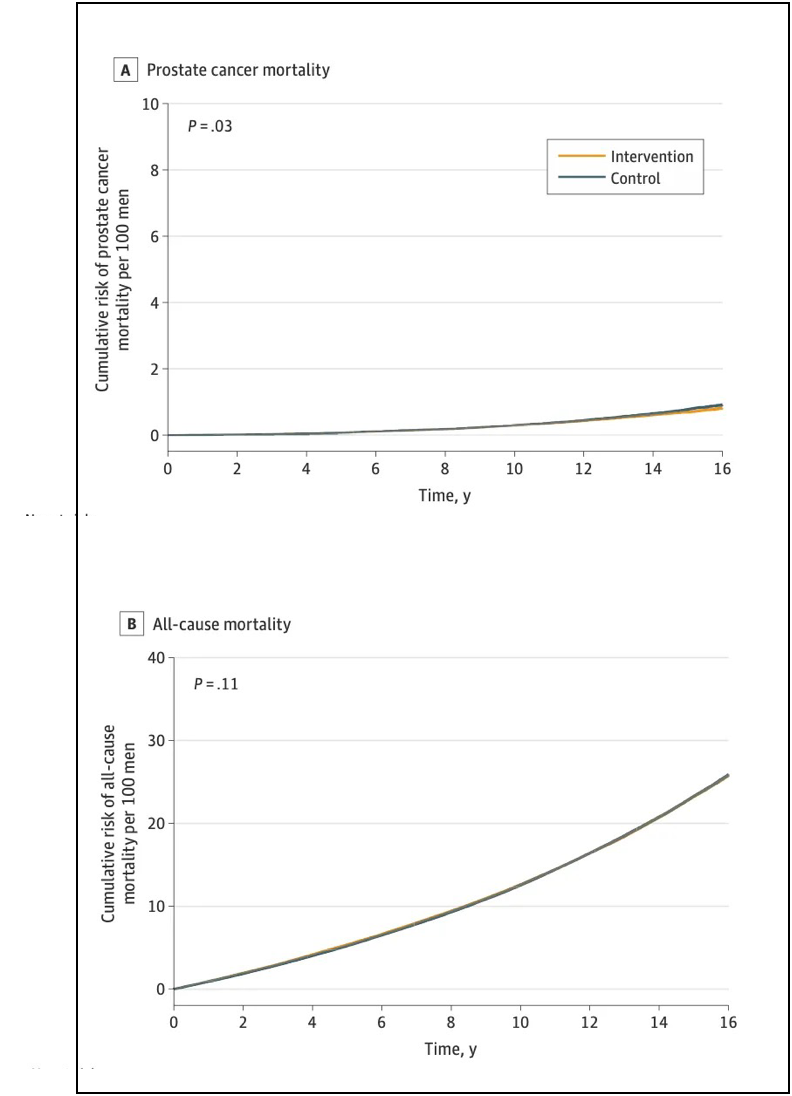
Let me explain what we have here. There are called “Kaplan-Meier curves.” Each graph actually has two lines, a yellow one, and a blue one. As time goes on (moving left to right) the rate of mortality from prostate cancer (top panel) and mortality from all causes (bottom panel) go up. If the intervention (prostate cancer screening) made a difference, there would be lots of daylight between the curves. The yellow line would be a lot lower than the blue line. As it is, you might not even be able to see two lines at all, because they’re right on top of one another, for the most part. (Malcolm Gladwell has a fun piece on Kaplan-Meier curves, of all things, except that they never show one!)
If you want to see a good Kaplan-Meier curve, check out the Covid-19 vaccine studies. Ok, I can’t resist. Look at these beauties from the Moderna and Pfizer trials.
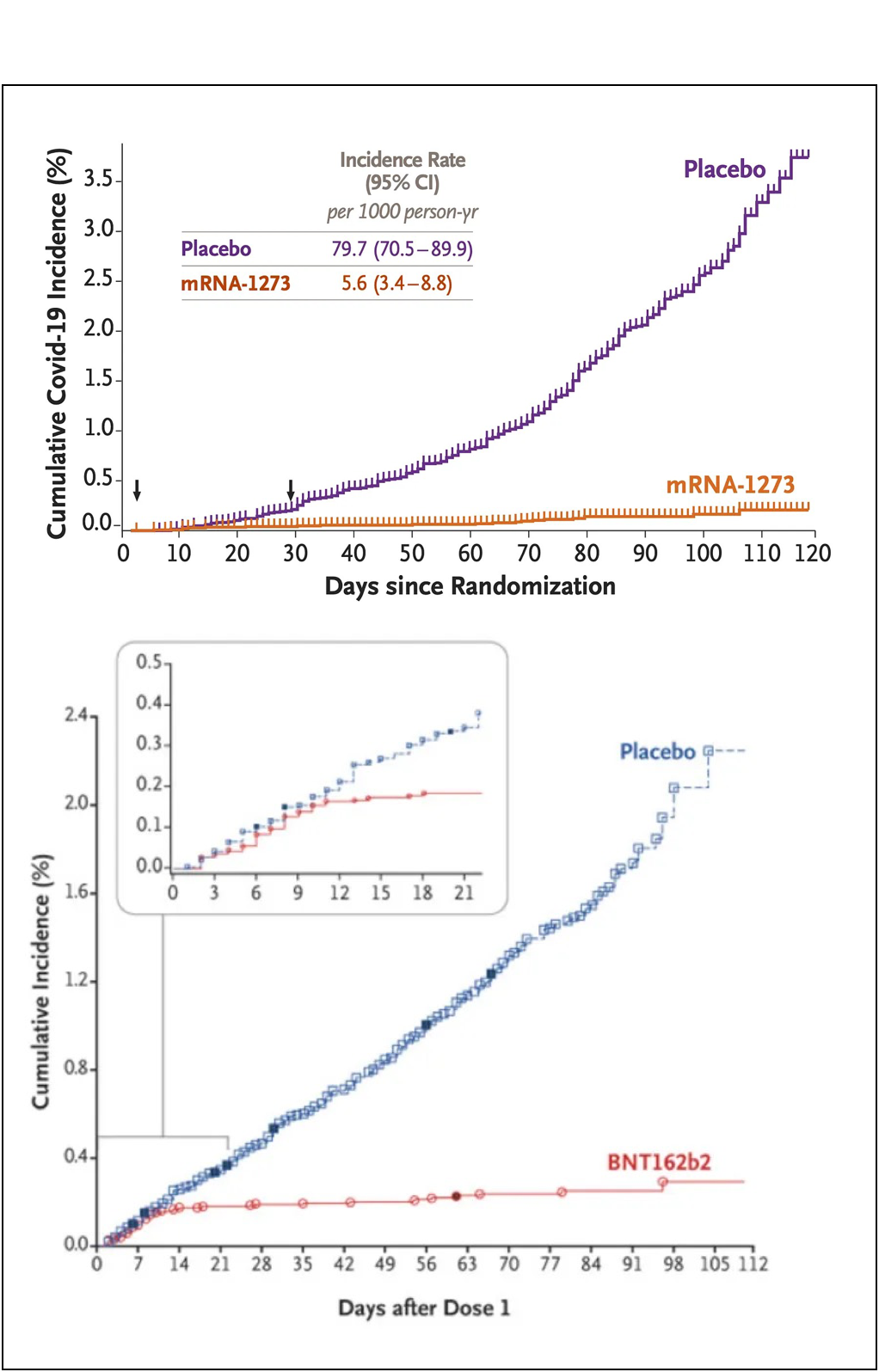
Mmm. Tasty. You could drive a truck through those Kaplan-Meier curves!
Back to prostate cancer. Technically, there was a tiny difference in prostate cancer mortality by about 15 years out. Around 1,100 men needed to be screened for one less prostate cancer death to occur. The rates of death from prostate cancer were 0.69% in the group that was invited to do screening, and 0.78% in the group that wasn’t. But there was no difference in all-cause mortality. That means that whatever harms come with cancer treatment (and let’s not downplay that), they actually offset the gains from early prostate cancer screening. Of course, those who get screened end up getting more biopsies, more surgeries, more chemotherapy, etc. That’s a lot of trouble for no difference in longevity
But as this last panel form the new paper shows, prostate cancer screening does succeed in finding cancers.

Indeed, there was separation between the yellow curve (people invited to get screened) and the blue curve at first. But, again, to what end? Screening meant more diagnoses, which led to more treatment, which in turn, always leads to complication; more time spent as patients hospitals, as opposed to people living their lives anywhere but.
This is all to say, the benefit of prostate cancer screening does not seem apparent to me based on these (and other) data.
The point of little takedowns like this is not to be nihilist for its own sake. It’s to spur action—to get researchers to look for something better. Prostate cancer is an important cause of mortality in aging men. It’d be nice if we had a screening protocol that genuinely prevented mortality in significant numbers. Right now, as is the case for so many cancers, we really don’t.
Chime in with your questions and feedback in the Comments section.
Prostate cancer screening is important for men who find that they have been identified with advanced PCa disease. If an annual PSA test had not identified a doubling of my PSA (PSADT), in all probability, I would be dead now. The big unanswered question in prostate cancer care and almost every other form of cancer is when did the cancer cells begin to aggressively mutate?
There are opinions that prostate cancer is a form of cancer with a thirty to forty year duration from start to it causing death. For a man whose aggressive prostate cancer begins to mutate while he is an adolescent, there is a good chance that without PSA monitoring that man would suffer an early painful death from the disease.
However, another man’s less aggressive prostate cancer might begin its maturation during his middle-age years, and if he is not having annual PSA monitoring, there is a statistical chance that this man will die with prostate cancer but not from the disease. Something else such as cardiac disease or another form of cancer such as lung cancer may kill him.
With circulating tumor liquid biopsies and better PSMA PET imaging, detection of prostate cancer within a man’s prostate gland at an earlier age might be detected before the prostate cancer has mutated and forced its way through and out of the prostate gland capsule and into the man’s vascular, lymphatic or nervous systems. Once the mutated prostate cancer cells have moved into those pathways, the cancer cells can travel through to the far reaches of the man’s body and become often a systemic incurable disease.
Early detection resulting from early testing and follow-up imaging is always a cost versus benefit analysis. It becomes most important for the patients with the aggressive cancer diseases seeking to make their ailments chronic instead of death sentences. This is something that medical economists and insurance actuaries discus during hospital budget debates, and the men with aggressive prostate cancer are never part of those debates. American medicine is a business first even though almost everyone tries to pretend and argue that it is not.
I literally cried tears of joy when I first saw those Kaplan-Meir curves from the COVID vaccine trials.