


Firearm deaths spiked in the summer of 2020 and after. What’s really behind it?
It’s not the pandemic, and it’s preventable.


Deaths caused by firearms reached 25-year highs in 2020, according to a new report from the Centers for Disease Control and Prevention (CDC).
Lest you worry that pandemic-related shutdowns were responsible for this, let me assure you this is not the case. As my research collaborative showed last year in the Journal of the American Medical Association (JAMA), homicides were initially unchanged at the outset of the shelter-in-place period in the United States, though rates crept up in the spring of 2020 before increasing dramatically in the summer. Peaking in July and August, homicides reached 127%–129% of their normal levels, amounting to over 1,000 more homicides those two months alone than statistical norms would have projected.
The CDC’s new report does not include data for 2021. But I pulled CDC provisional data to see how things developed, and 2021 looks to have been even worse than 2020.
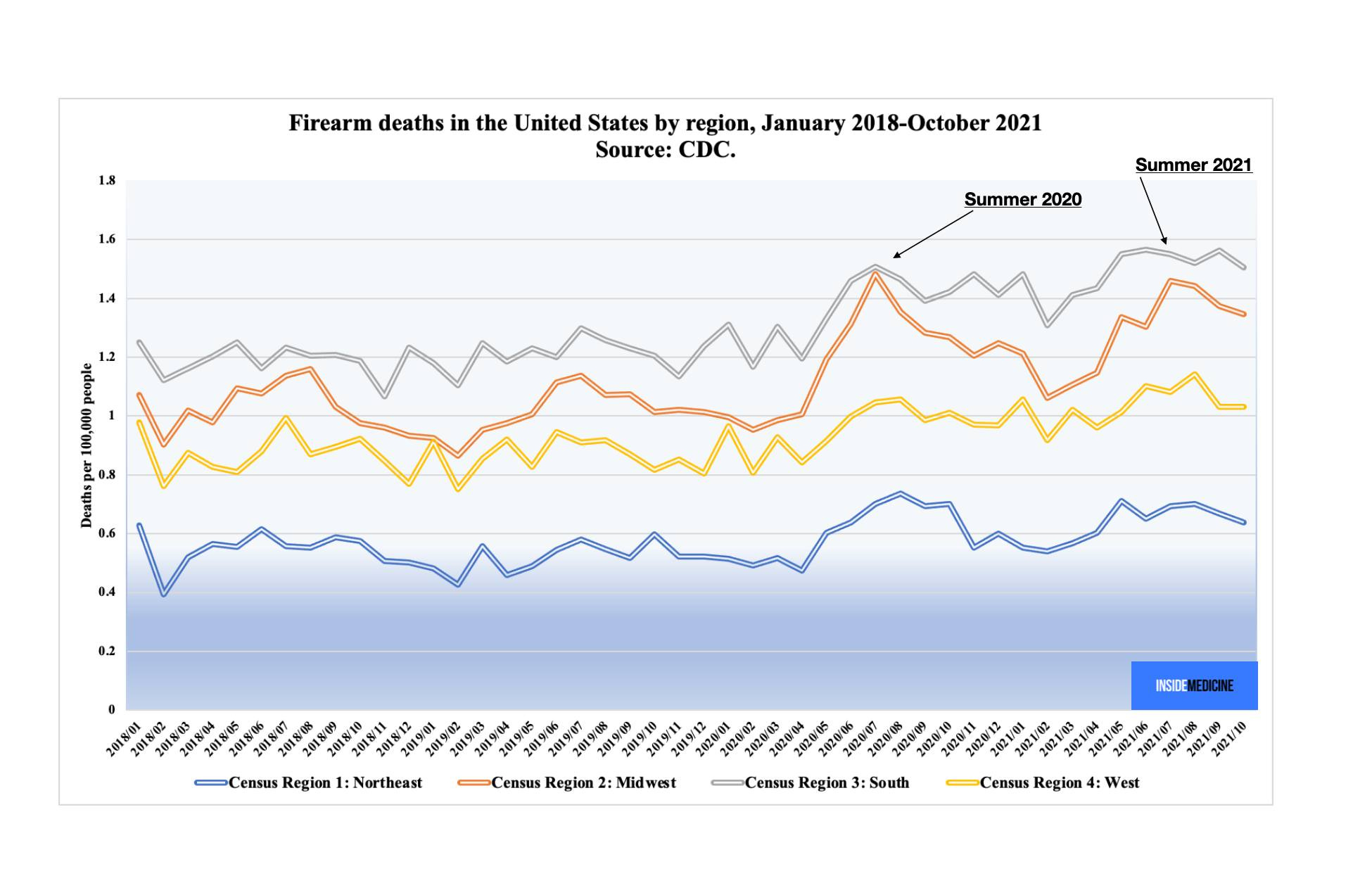
CDC data show a sudden increase in firearm deaths in the months after the Covid-19 shelter-in-place ended.
What’s behind all of this? A number of factors. But one thing we can say is that the increase in homicides does not appear to have been driven by pandemic overreaction, as many will likely try to claim. We know this because most of the homicide increases occurred in the South and the Midwest, regions that did less to stop Covid-19, in comparison to the West and the Northeast, regions where pandemic mitigation measures were observed longer, and also ones that entered 2020 with lower baseline homicide rates. Large increases occurred in cities, which might reflect changes in law enforcement (and that might be pandemic related), but also in rural and non-metropolitan areas.
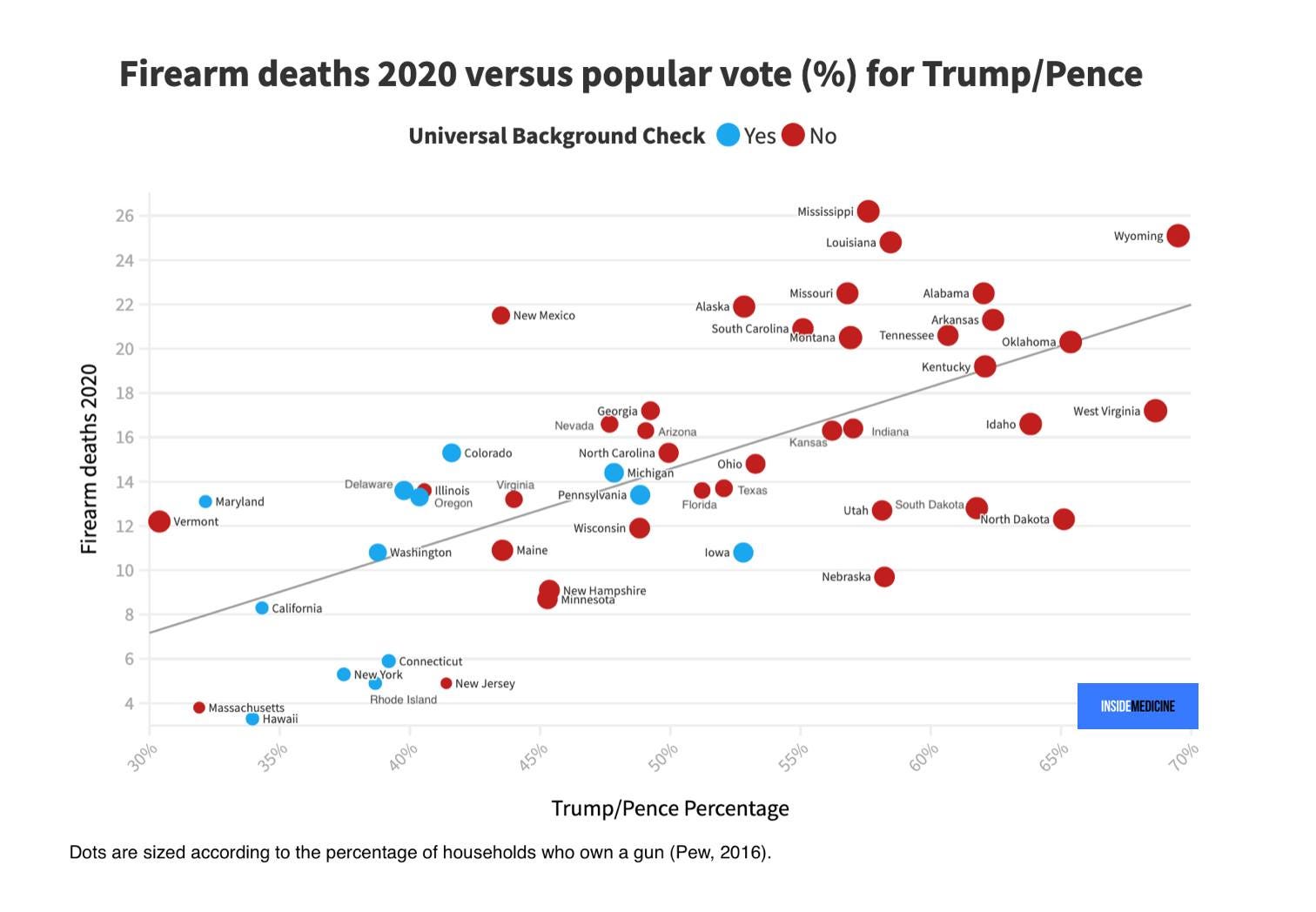
State politics play a huge role, it appears. States with higher rates of gun ownership have higher rates of firearm deaths. States with universal background checks have lower rates of firearm deaths.

State laws and voting patterns correlate to firearm deaths. (Image by Jeremy Faust and Benjy Renton for Inside Medicine. Data: CDC, Pew, MIT election lab).
And national politics seem to matter too. If nothing else, voting results are an interesting proxy for a group of behaviors and cultural forces that feed into a culture of gun violence. As the graphics we made for Inside Medicine show, states that voted more heavily for the Trump/Pence presidential ticket in 2020 had markedly higher rates of firearm deaths in 2020 than those going for Biden/Harris. (The red state–blue state divide on firearm-related deaths is not a new thing.)
The previous graph with voting patterns and gun ownership swapped. (Image by Jeremy Faust and Benjy Renton for Inside Medicine. Data: CDC, Pew, MIT election lab).
The CDC, of course, isn’t going to “go there” and there’s much to say, outside of politics. “The substantial increase in firearm homicides and suicides are important public health concerns,” said CDC Acting Principal Deputy Director Dr. Debra Houry, via email to Inside Medicine. “It is also critical to understand the widening inequities by race and ethnicity as well as by poverty level. By understanding and addressing the drivers of these complex issues, we can provide needed tools to create healthier and safer communities.”
Writing in JAMA today, Houry also noted that “counties with higher poverty levels already had the highest firearm homicide rates, and these counties also experienced the greatest increases.” Meanwhile, Black and American Indian/Alaskan Native populations had disproportionately higher rates for homicide and suicide, respectively. Houry and her coauthors also pointed out that medical schools don’t teach about screening patients for firearm risks, which is a mistake; conceptualizing firearm safety just as we would any other kind of risk factor for poor health outcomes is useful, they argue. Just as physicians can effectively counsel patients to quit smoking to avoid heart disease, healthcare professionals have been shown to be able to decrease downstream violent injuries and incarceration by engaging youth in counseling that amounts to a kind of preventative care.
•••
According to Dr. Megan Ranney, an expert on gun safety, laws can and do make a difference. During a brief conversation last night, she pointed out to me that in states which have loosened gun laws, many adolescents and young adults have paid with their lives in the aftermath. But she has also written that increases in firearm deaths in states which pulled back from gun safety laws might reflect the cultural shifts that in fact led to the legal changes, as opposed to the laws themselves being the drivers of increases in firearm-related deaths.
To untangle all of this, firearm violence research must be funded, just like any other public health menace might be. And the CDC’s new report is an example of that. Until a few years ago, the CDC was routinely allocated exactly $0 per year to study firearm violence. Finally, Congress infused the CDC’s Injury Center with $12.5 million earmarked for this type of work. Today’s report is actually the first time that the CDC has published a report like this, and it comes as a direct result of that funding. So in the midst of a lot of bad news, the fact that there is public funding for firearm violence epidemiology is a small step in the right direction. (It’s said that funding earmarked for these purposes may actually increase in the coming fiscal cycle, but that obviously remains to be seen.) Meanwhile, the CDC is not permitted to advocate for gun control in any way, shape, or form, including even commonsense policies like background checks, which have been shown to reduce firearm deaths. That’s due to a rider which was added to a budget bill in the 1990s, the so-called Dickey Amendment. So, while the CDC is not permitted to advocate for even the slightest modicum of gun control, it can at least advocate for firearm injury and homicide prevention via other methods, such as medical education, funding for youth and young adult counseling, and the publishing of important, if unsettling, public health data.
•••
Dear Inside Medicine Readers! Want more? Then please join me as a Premium Content subscriber and go "Inside" Inside Medicine. Benefits include exclusive articles and a members-only Facebook group where I'll answer your questions and hold interviews with major names in medicine and health, and share more about my work as an ER doc. It's a growing community of wonderfully engaged people who want to connect with me, other experts I trust, and each other. I hope you'll join me: https://insidemedicine.bulletin.com/subscribe. Thanks!
•••
❓💡🗣️ What are your questions? Comments? Join the conversation below!
Follow me on Twitter, Instagram, and on Facebook and help me share accurate frontline medical information!
📬 Subscribe to Inside Medicine here and get updates from the frontline at least twice per week.
Acknowledgements: Dr. Megan Ranney for expertise and insights; Benjy Renton for data acquisition and images.