


FDA moves towards monovalent Covid-19 boosters this fall.

Yesterday, the FDA’s vaccine advisory panel met to discuss the latest data and fall booster plans.
Going into this, there were many questions—and we got some answers.
Will fall boosters be Omicron-only?
Yes. As some experts have argued (and as I’ve written here), encoding the Wuhan spike protein in the vaccines is no longer necessary, and probably has downsides related to immune memory. We keep teaching our immune system to expect the Wuhan version of Covid-19. That virus is long gone. It’s time our vaccines fully reflect that. Now they finally will.
Are bivalent boosters waning?
Yes and no. Clearly with respect to infection, the boosters wane. The CDC presented what we call surrogate data for that question by showing us the difference between booster dose effectiveness against hospitalizations (which could include some mild illnesses) and critical illness (which included death or ICU). There was substantial waning of protection against all Covid-related hospitalization, but less waning with respect to critical illness. In fact, adults who had a bivalent dose an average of 146 days prior had around the same protection as those who received monovalent doses an average of 381 days prior. Leaving aside the uncertainty of the methods the CDC is using here (we won’t go that Inside Medicine today), that tells me that even the bivalent antibodies fade away after a boost fairly rapidly, leaving vulnerable populations susceptible to Covid tipping them into the hospital—be it solely due to Covid, or due to an exacerbation of an pre-existing medical condition. But the few remaining antibodies (and other immune cells augmented by boosters), continue to provide added protection for at least 4-6 months. That said, once again the protection added by the bivalent boosters an average of 146 days out is pretty similar to the monovalent’s continued protection 380 days out.
All of this tells me that, as I suspected and wrote previously, the bivalent booster was not a massive improvement over the monovalent original. What matters is that high-risk people stay up-to-date.

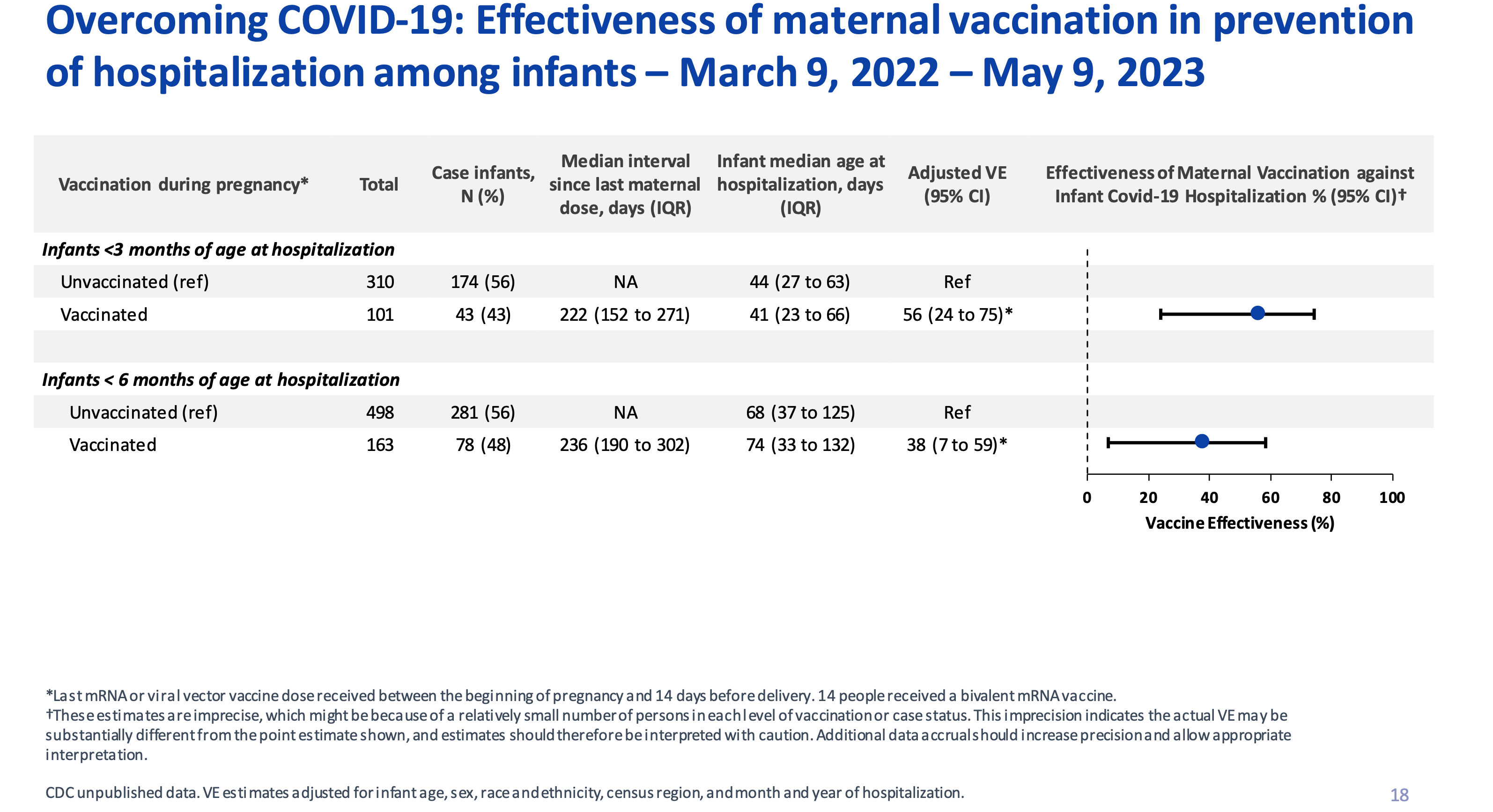
Update: Do vaccines help in pregnancy and provide infants with downstream protection?
While I’ve long felt that boosters for young and healthy people were likely not needed (and possibly problematic, if only very rarely), the one young demographic subgroup I’ve felt is underboosted and deserves better policies are those who are pregnant. (Here’s a piece I wrote on this point last year in a respected medical journal with Dr. Sonja Rasmussen and Dr. Denise Jameison—two experts in this field.) We already had data showing that pregnancy was a dangerous time and that infants born to mothers who vaccinated or boosted during pregnancy were less likely to be hospitalized as far as 4 or even 6 months into life. The CDC added more data to this, clearly showing that timing counts. I would continue to recommend anyone who is pregnant get a dose of Covid-19 vaccine during the early 3rd trimester. This would maximize protection during the most dangerous time of pregnancy and give the eventual infant a longer tail of protection than if the mother had gotten a dose earlier in pregnancy. However, as of now, pregnancy is not a condition for which an additional dose is permitted by the FDA and CDC. So for women who happen to be pregnant this fall, they’ll be able to get a dose to help them and their infants. But for those who are not pregnant who get a dose in the fall but then become pregnant later, an additional dose (say next spring or summer) during that pregnancy is not allowed. That’s bad policy and we should fix it. Previously, Dr. Peter Marks (the FDA’s lead on vaccines) told Inside Medicine this might change. It hasn’t yet.
Update: How are the bivalent vaccines performing in the immunocompromised?
Overall, the news here is similar. Protection against infection (using the gulf between all-Covid hospitalizations and critical cases as the surrogate for this question) seems to wane quickly. But protection against critical illness did not wane as much, matching the pattern exhibited by immune-intact persons. This aligns with data and analyses I collaborated on with Israeli epidemiologists. We found that the pattern of waning is not that different when you compare immunocompromised to immune-intact people. It’s just that immunocompromised people have much higher risks. In other words, if the booster’s effectiveness starts at 70% for both groups, the absolute effect is much more prominent in the immunocompromised. One way to think of this is to imagine that the rate of hospitalization among immunocompromised people is, say, 5% (1 in 20). A 70% decrease of 5% would bring the rate down to 1.5%. That means that after the boost only 1 in 67 immunocompromised people would be hospitalized. But if the unboosted hospitalization rate among the immune-intact starts at 0.5%, the boost drops it to 0.15%, or 1 in 667. That means that waning has much larger implications for the immunocompromised. On this basis, I continue to support frequent boosting for the severely immunocompromised.
Will monovalent Omicron-only boosters really improve things?
Yes, for some people—and especially high-risk and older people. That said, I continue to believe that the value-add for additional boosters for the young and healthy people boosting is not apparent, other than a short-term decrease in infections. In my work with epidemiologists in Qatar, we showed that people without high risk did not get any added protection against severe Covid from even a 3rd dose (that’s how good the two-dose series was for the young and healthy!), and that eventually the rate of reinfection in the boosted began to exceed that of the unboosted (a phenomenon called immune imprinting). There are some reasons for these groups to get boosted (such as temporarily protecting close contacts from infection), but until now I’ve been worried that the short-term benefit of boosters in young and healthy people has been short-sighted because of the imprinting issue (and even the low rates of myocarditis in young males in particular). If the imprinting problem is neutralized by moving to an Omicron-only vaccine, that’ll be good and welcome progress.
Therefore, I believe that a monovalent Omicron-only booster (created to code the spike protein of the most recent dominant subvariant that we can) will indeed help decrease booster waning (barring some new awful variant). This is for two reasons. First, a vaccine better matched to what’s circulating will fight the virus better in the early days, weeks, and months after the dose. Second, dropping the Wuhan portion of the vaccine will decrease the immune imprinting that we’ve seen crop up, in which we accepted short-term protection in exchanged for longterm higher rates of reinfection. (I discussed this on the PBS News Hour this spring).
One complaint about batching data.
I’ve long felt (and written here) that the vaccine manufacturers (and even the CDC surveillance networks) have overplayed the effectiveness of the “boosters for all” policies by batching and reporting data for people ages 18 and up as one big group. lumped together, rather than teasing out the age groups (say ages >65 years and up, 18-64, and 0-17). The result of batching all ages together is that the data appear to show boosters as being more effective for young adults than they really; simultaneously, this approach makes boosters look less effective than they are for older and sicker people. The bivalent booster is indeed a very useful and important thing for older and sicker people. But we have solid data showing that the number of bad outcomes the bivalent booster prevents in young healthy people is exceedingly low.
Again, most of the data we saw in the FDA’s meeting yesterday repeated this problem. Meanwhile, the CDC made a point of how low booster uptake has been lately. In my view, the solution is to worry less about booster rates in young and healthy people and to redouble our efforts to reach older and immunocompromised people.
To understand this, consider two hypothetical options.
Option 1: 95% of immunocompromised and other extremely high-risk people (a minority of the population adding up to say 20% of the population) get another dose but just 30% of the rest of the population gets one.
Option 2: 75% of all people get another dose.
While it might seem scary to choose option 1 (because a much smaller segment of the overall population gets a dose), from the standpoint of the number of bad outcomes avoided, it’s actually the better one.
So when people ask me if I’m worried about low booster rates, I say that I’m worried about low booster rates in high-risk individuals. That’s where our focus—and our messaging—should be centered.
From Mark Zuckerberg on being asked to lie for the government just this week,
Dr Faust, I’m curious about your thoughts on what Mark Zuckerberg said this week that he was asked to censor true things by the government, here is the full quote, how are we supposed to trust these agencies when it’s clear they are captured by the pharma companies, it’s really complicated
“Just take some of the stuff around Covid earlier on in the pandemic, where there were real health implications, but there hadn’t been time to fully vet a bunch of the scientific assumptions. . . Unfortunately, I think a lot of the establishment on that kind of waffled on a bunch of facts and asked for a bunch of things to be censored that, in retrospect, ended up being more debatable or true. That stuff is really tough, right?”
Noted, monovalent, omicron only.