


Does live video improve outcomes in one of medicine's most harrowing procedures?
New data suggest that video technology makes putting patients on breathing machines safer.

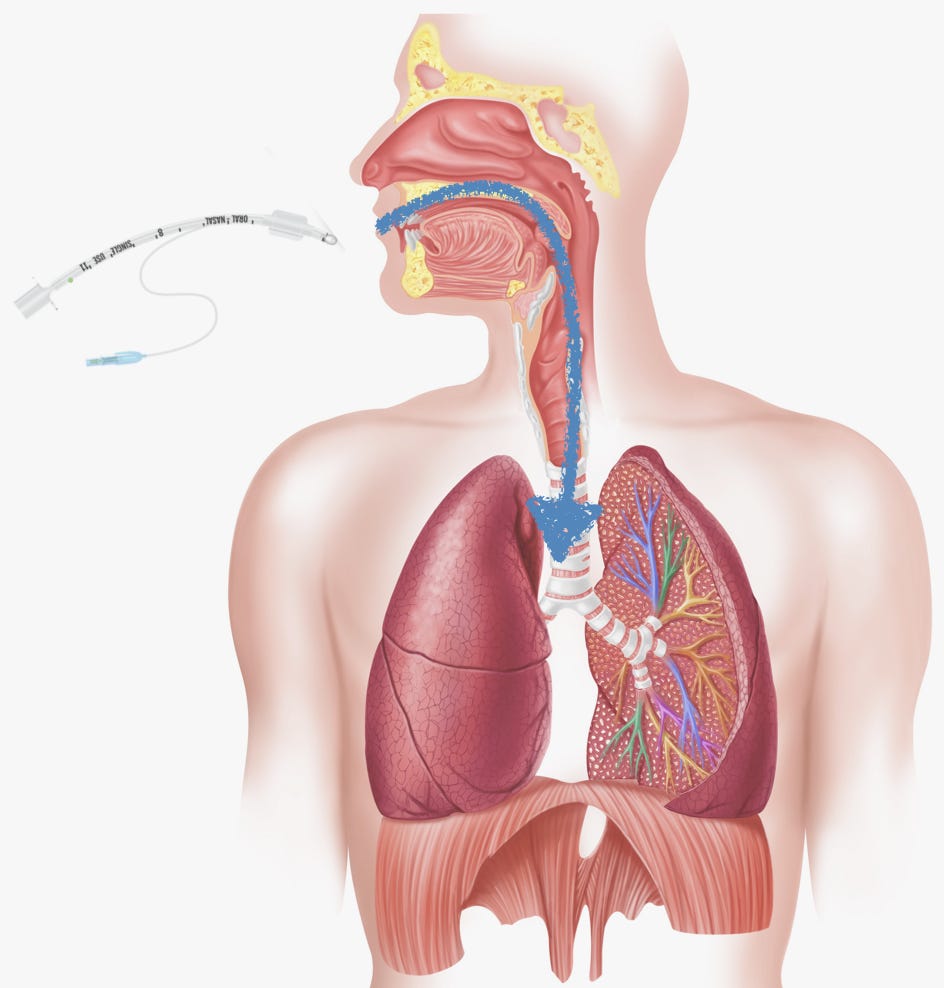
The idea is simple enough: Get the small plastic tube into the mouth, past the uvula (that bulbous thing that hangs down at the back of your mouth), between the vocal cords, and into the trachea. The tip of the tube should end up a couple of inches above where the trachea (a.k.a. the windpipe) splits in two, one for each lung. Once achieved, you connect the top of the tube to a breathing machine (a ventilator) that supplies oxygen.
I don’t know if that sounds easy or not, but this procedure, known as endotracheal intubation, is a key skill for any emergency or intensive care physician. Intubating a patient proficiently and quickly can be the difference between life and death for a critically ill patient.
It takes a whole team to do this correctly. But as an emergency physician, it is my job to physically get that tube into the trachea so that oxygen can be delivered to the alveoli in the lungs, allowing oxygen to get into the blood.
As soon as cameras got small enough to affix to the leading edge of the device used to open the airway (called a laryngoscope, pronounced “luh-rin-juh-scope”), technophile doctors started trying to make it work.

Making live video feedback standard, it was hoped, would negate the need to perfectly line everything up to enable a sightline from a patient’s open mouth all the way to their vocal cords. Here’s a diagram of the setup needed for intubation without video assistance.

Now, there are a number of techniques and tricks that make the sightline I need to intubate without video possible. During my training, I took this very seriously. So whenever I intubate today, I treat every single case as if it could be the most difficult one I’ve ever encountered—even if it looks like it will be an easy one. Most of the tricks I deploy boil down to optimizing the geometry and ergonomics. The more time I spend optimizing my work environment—correctly positioning the patient and me—the easier things will be.
I take this to such extremes at times, that I can almost sense the eye-rolls from impatient trainees I might be working with, let alone seasoned nurses and respiratory technicians who have done this procedure countless times. Of course, when things go exceedingly smoothly, everyone feels vindicated. I am pleased because I know that my “over-the-top” preparation had a lot to do with guaranteeing the “easy airway.” Meanwhile, I suspect my colleagues might secretly be thinking, “Why all the fuss? That was an easy airway!” To that, I say…exactly!
The debate gets settled.
In the 25 years since the first video-assisted intubations were performed, the technology has advanced. Nowadays, the best views of the airway are often not attained by looking directly into the mouth with the naked eye, but rather, by putting a video laryngoscope into the airway, and looking up at a nice portable color video screen conveniently situated just a foot or two away.
Still, a debate raged in the emergency medicine and ICU community over which way was best: Old-school (no camera) or new-school (with camera) intubation? The Luddites argued that old-school intubation was a necessary skill; “You never know when your camera will malfunction, or when you might be in a situation without such niceties.” The tech-lovers argued that the benefits of 21st century gadgetry would make it worth the expense and that loss of the “old art” was not a big one. Do you really need your Uber or Lyft driver to be able to drive a stick shift, if all the cars are automatic? Moreover, the views that the camera sometimes creates can be astoundingly good.
A trial recently published in the New England Journal of Medicine has basically ended the video versus non-video debate. The techies won. When video was used, the procedure was successful on the first attempt 85% of the time, compared to 71% when video was not used. While there was no difference in complications, that difference is still meaningful, especially since video use made the procedure faster.
Interestingly, the difference in success rate between video and non-video use was greater among the least experienced participants. That is, those with less prior experience had a far higher success rate when using a video-assisted device. The more experience the physician had, the smaller the difference in video vs. non-video success rates were.
A reversal on teaching.
For a long time, the conventional wisdom for teaching intubation to trainees went something like this: teach trainees how to intubate without video assistance first. Then, once they have mastered the old school way, permit them to have the advantages offered by the video assistance.
This tested the nerves of supervising physicians like me. After all, if a resident I am training is intubating a patient without video, it’s almost impossible for me to see what’s going on in there. I have to rely on what the resident is telling me. (Describing what you’re seeing when intubating is its own art, kind of like the play-by-play commentary of a sports radio announcer; painting an accurate picture seems easy. It isn’t.) In the last decade or so, some teachers have split the difference by allowing the trainee to intubate with a camera on the tip of the laryngoscope, but not allowing them to see what’s on the video screen. The idea was to give the learner the experience of old school non-video assisted intubation without foregoing the safety provided by the teacher’s ability to watch everything live on the video screen.
But it turns out that this is unnecessary. In fact, many experts (including one of my mentors, a well-known ER/ICU doctor) now argue that the best approach is to give learners every tool possible at first in order to maximize success—including video. Then, once accustomed to the anatomy and the procedure itself, learners can begin trying to intubate without video assist (albeit with a video-enabled device on hand, ready for use at any time). Indeed, those Luddites had a point: it is good to know how to intubate without video laryngoscopy, in case the device fails (or is not an available resource) or in instances when, ironically, video is making the procedure harder.
Changing my own practice.
I first learned to intubate without video assistance. Then I learned to use the video, and eventually became reliant on it. But late in my 3rd year of residency, a mentor of mine challenged me to stop using the video. By then, I’d intubated a lot of patients, so I knew what I was doing. Still, the thought was scary, especially since he wanted me to use a laryngoscope that had no camera. But knowing I had back-up (my mentor and a video-enabled device nearby), I tried. I made sure to optimize everything, just like I wrote above. Everything went perfectly. In fact, it was exhilarating. I loved being in control of the procedure and I loved that nobody but me could see what was going on in there. It was “my airway.” The pressure of everyone in the room being able to see everything on the video screen in real time (and make “helpful” comments and suggestions) was gone.
From then on, as a matter of pride, I intubated without video in almost all cases. I even encouraged the newer residents I train to do the same, carefully making sure they knew just how to describe the action ahead of time, so that the room would not lose confidence in them and force me to take over the procedure. (The 20 to 80 seconds it takes to do most of these can feel like an eternity without video or a good play-by-play.) I also taught them all the tricks for getting a great view of the airway without video.
The data are in. I need to stop doing that. From now on, I’ll teach the less experienced residents using the full luxury of the video-assisted device. Then, once I know they’ve mastered that, I may challenge them to use the video less.
This might mean foregoing the facilitation of a few moments of triumph for the residents. I’ll miss that. But the end user is not the doctor-in-training or me: it’s the patient.
You nailed it!
Very helpful for family caregivers with medical POA's! Thank you.