


Covid-19 metrics update, August 28, 2023.

Just a quick data snapshot from the Inside Medicine Covid-19, flu, and RSV dashboard.
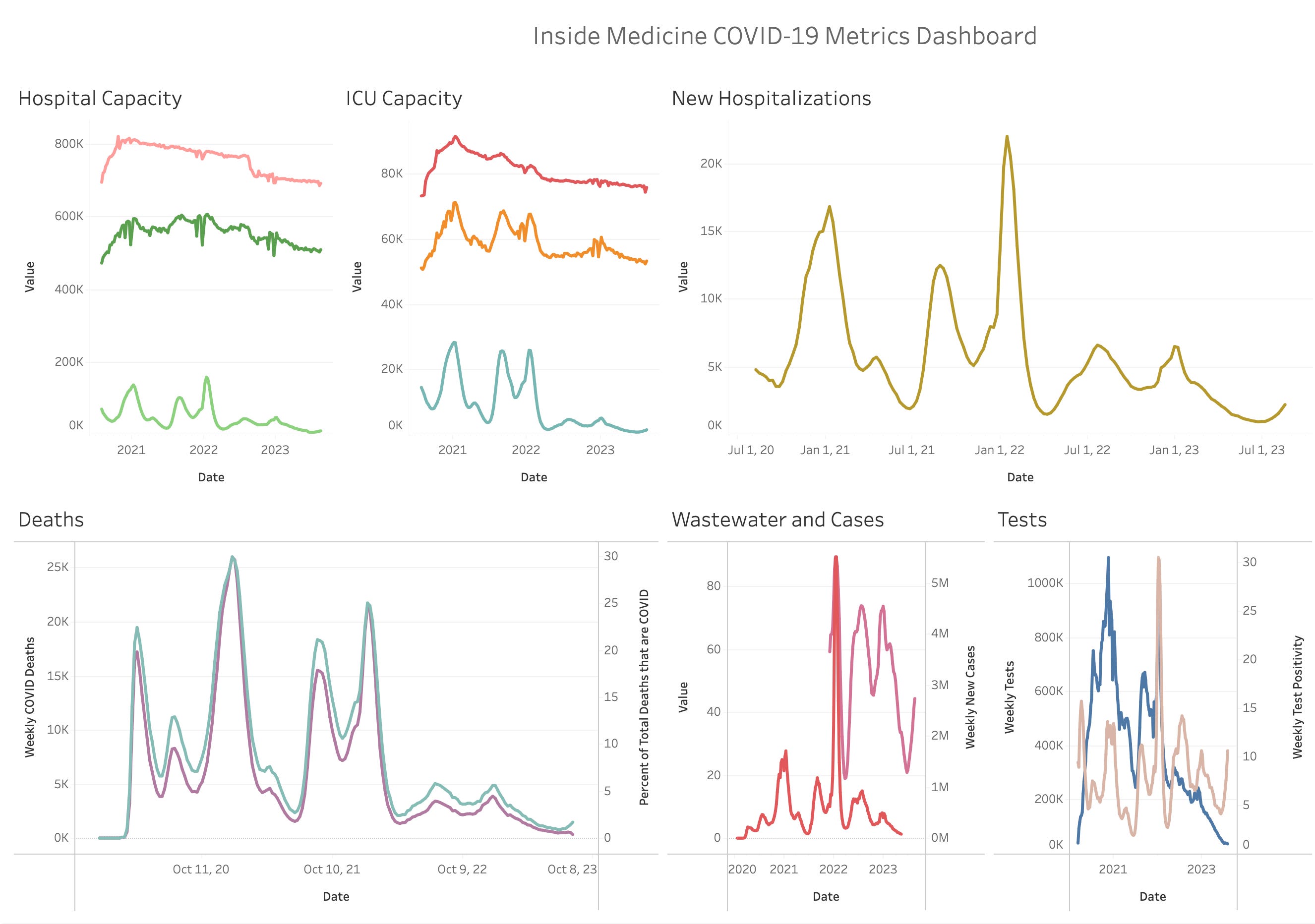
Overall, there has been an uptick in Covid-19-associated hospitalizations in recent weeks, as you’ve probably heard. Fortunately, these increases are nothing like past waves. On the other hand, as you can see in the graph below, influenza and RSV are associated with essentially zero hospitalizations at this time of year. So, for Covid-19 to be doing this at this time of year—almost 3.5 years after the first bad US wave—is impressive.
Now this does not necessarily mean we are in for a worse fall or winter. There are too many unknowns to predict that. What it does say is that Covid seems to be able to persist, at least at some level, during the summer months. It’s happened every summer since this all began. If it weren’t for the Delta variant disrupting things in the summer of 2021, the seasonality of this pathogen would be even more apparent than it already is. Still, it is a little unsettling, philosophically if not epidemiologically, that this virus can hum its way through the summer months and never disappear. Again, flu and RSV just aren’t known to do that.

The relatively good news is (as you can see above) that the recent increased hospitalization numbers are nothing like early Omicron, or even the heart of flu season (2018-2019, 2019-2020, and 2022-2023; remember, we knocked flu and RSV out for two winters, thanks to Covid mitigation). The numbers aren’t even as bad as last summer, though some of this could be detection bias (less testing in hospitals). So, as you can see below, most states are seeing Covid-19-associated hospitalizations that are 10% or less of their own maximums.

Hawaii is one place where rates are closer to its all-time high. This by the way does not appear to be a statistical artifact due to increased hospitalizations from the Maui fires (i.e. people getting tested for Covid who were admitted for burns, for example), as coronavirus wastewater levels began to rise there in late July.

Again, some of these numbers depend on the various testing strategies in hospitals. Unlike in the past, not all patients getting admitted to the hospital get a Covid test automatically. That’s why it’s good to track a variety of metrics to get a sense of what’s happening in a particular community.
To see how yours is doing, check out the Inside Medicine Covid-19 metrics dashboard.
Questions? Comments? Share below!
Thanks to Benjy Renton for curating the data for our snapshot and keeping the dashboard up and running.
I applaud your time consuming efforts to keep us informed. I'd still appreciate better info on what data and the source of that data is used in your graphs- especially for deaths. If the latter is from the CDC website I'd appreciate it if you could help navigate their site to what stats you are relying on. The fact that the CDC stopped reporting deaths after the Emergency was declared over calls into question the quality of their reporting. They also changed the way expected deaths were forecast to include pandemic related deaths, which of course reduced "excess death" reports. The rationale for this obfuscation is poorly described by the CDC. Most people I know would say that I am not a stupid person but I find it incredibly hard to find what I'm looking for on the CDC website and to fully understand it when (I think) I have located it. And their search function is almost useless. Help please.
As always, appreciate your time spent in data, analysis, and communication! I still worry about accuracy of data (not you) as fewer people test now in terms of cases, and hospitals can and do put down cause of death or even hospitalization as the comorbidity which patient may have been managing fine until they got COVID. There doesn't seem to be a correlation between states that have highest amount of cases and states with highest amount of hospitalizations. And it's pretty clear that COVID caused much $$ loss for hospitals and the managing industry as they lost patient visits, tests, elective and non-elective surgeries due to fear of COVID. Seeing really bad related outcome of poorly administered medical services in Western MA due to reduced staffing, reduced patient time, poor communication, and reduced access to long time docs. Never mind that we are in an election year and with patients, general population, and medical folks suffering from pandemic fatigue, no candidate or party wants to touch the subject. I also feel as a severely immune-compromised person with loved ones also immune-compromised that we can't live in that bubble that says COVID is "gone" as a serious issue until we see a lack of a fall/winter COVID surge...which hasn't happened yet. Thanks for your vigilance.