

A near-miss on a United 777 offers an important reminder for medical professionals.
A near-miss on a United 777 offers an important reminder for medical professionals.
It's the communication.

Physicians in ERs and intensive care units look to the aviation industry with admiration. If only medicine could develop a culture of safety and communication as superb as our commercial aviation counterparts, we often say, fewer mistakes would be made, and lives would be saved. (That said, research that suggests medical errors lead to high fatality rates is hopelessly flawed, despite being irresistible clickbait for medical journals and the media in general.)
Whenever a major accident—or even better, a narrowly-averted one—occurs on a commercial jet, I’m always interested in learning what caused the problem and what the pilots did. As an ER doctor, the National Transportation Safety Board reports and the cockpit recordings provide me with unusual opportunities to see how my peers in a different profession respond to pressure, and keep their cool as they troubleshoot a problem in just a few seconds.
A recent near-miss incident in the aviation industry looks to have been an exception—where the usual culture that ensures safety was not followed. While nobody was hurt, an apparent lapse in normal communications almost proved devastating.
Communication’s the key.
One of the hallmarks of successfully averted disasters is calm and clear communication. Like in medicine, aviation lingo is efficient. One of the most consistent features that reflects the culture of safety in aviation is “closed-loop communication.” Here’s an example:
Chicago Air Traffic Control: "United 450, please descend and maintain 23,000 feet."
United 450 Pilot: "Descend and maintain 23,000, United 450.”
Notice that the call sign, United 450, comes at the start of the Chicago transmission, and at the end of the United transmission. That’s intentional. Chicago is radioing dozens of planes. By starting with the call sign, it’s clear which plane the message is intended. By simply repeating the command back, the pilot confirms that the instruction has been heard, verifies the specific details, and states that the cockpit will comply. The pilot ends the message with the plane’s call sign, both to relate that the message has been received by the right recipient and that the transmission is complete. Not a wasted word!
A recent near-miss, explained.
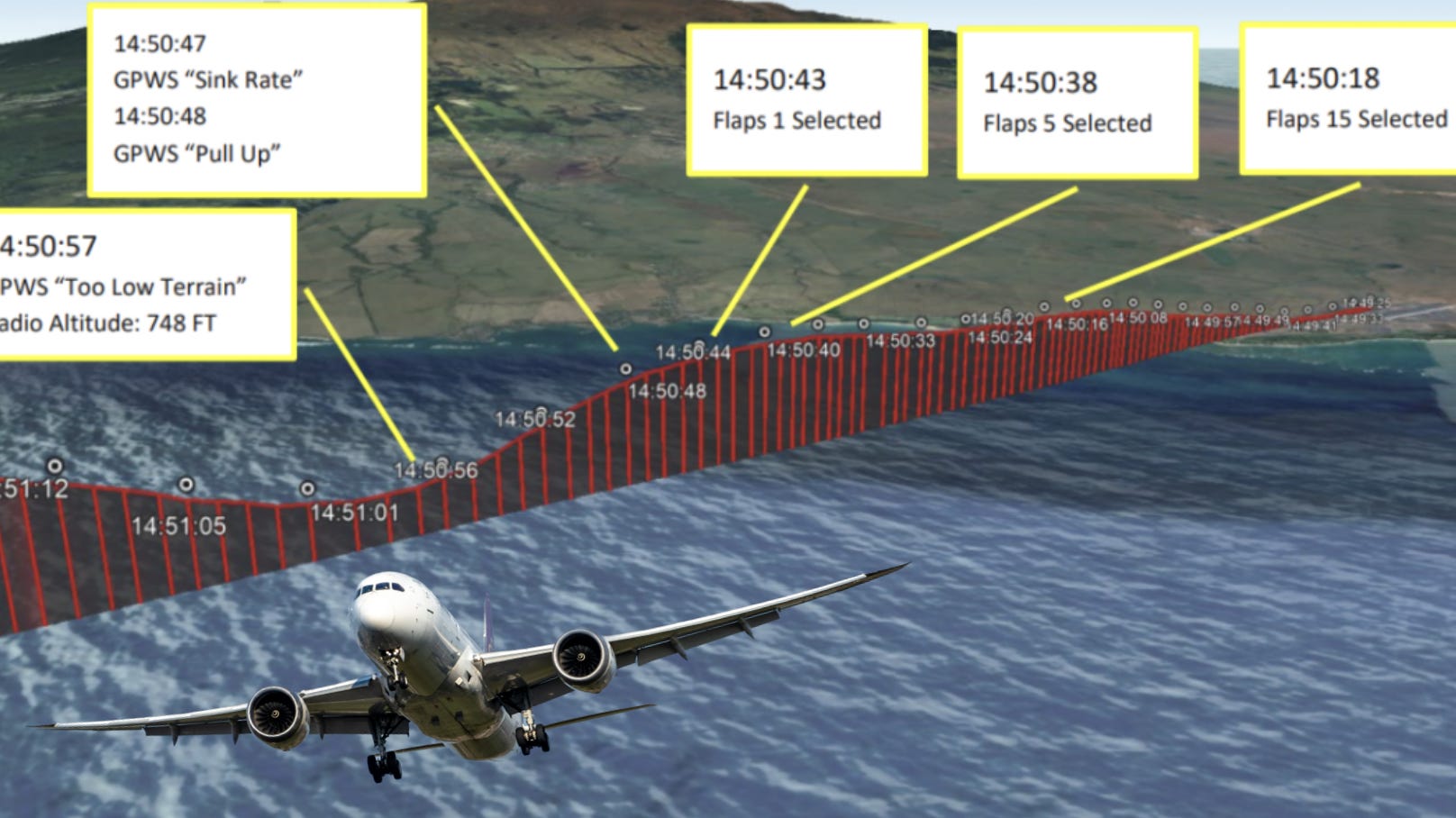
Last year, a Boeing 777 departed from Maui’s airport, headed for San Francisco. Due to some turbulence, some adjustments were made on takeoff. But something went wrong and the plane suddenly and rapidly descended from an altitude of 2,100 feet to just 748 feet in a matter of seconds. If the cockpit hadn’t sorted the problem out, the plane would’ve ended up in the water a few seconds later.
What happened? Miscommunication. The pilot wanted the flaps set to 15°. The co-pilot heard 5°. When the flaps went to 5°, the plane headed towards the ocean, rather than the sky. Fortunately, the team figured out the mistake quickly. The time it took from when the wrong flap settings were selected until the jet reached its lowest point—just 748 feet above sea level—was 18 seconds. Most of the descent occurred in under 10 seconds. Sounds terrifying.
While there is no flight recording—the pilots did not initially report the incident because it somehow did not meet official reporting requirements—the cause of the event has now been officially been determined by the National Transportation Safety Board to have been miscommunication between the pilot and co-pilot.
So, while we don’t know exactly what was said, the pilots seem to agree that the miscommunication occurred.
It seems to me that the usual closed-loop communication did not occur. If it had, the mistake would have been caught before the plane began its plunge towards the Pacific Ocean.
Here’s how it might have gone…
Pilot: Set flaps to 15 degrees.
[Co-pilot says nothing, and sets flaps to 5 degrees].
Assuming the co-pilot said nothing in response, the miscommunication had no chance of being caught before the change was implemented. But if the co-pilot had completed the closed-loop communication, here’s what could have happened instead:
Pilot: Set flaps to 15 degrees.
Co-pilot: Flaps set to 5 degrees.
Pilot: Negative. Set flaps to 15 degrees; one-five degrees.
Co-pilot: Roger, setting flaps to 15 degrees. That's one-five degrees.
Crisis averted.
How doctors—and you—can benefit from improved closed-loop communications.
I rely on closed-loop communication with my colleagues when taking care of very sick patients for whom seconds matter. Let’s say a nurse is asked to give a patient 2 milligrams of lorazepam intravenously (an anti-seizure medication). Here’s how it might go:
Nurse: I’m now pushing 2 milligrams of loraz’ IV.
Me: Thank you, 2 migs intravenous lorazepam.
Now, you’ll notice some things here. I did not just repeat the information back verbatim. Each small change had specific purpose.
Let’s deconstruct.
I start with “Thank you.” This has two purposes. First, I mean it. Thanks! Second, it’s a way of saying “I am closing the loop on your communication to me.” It’s my way of saying my call sign. (It might be weird if I said “2 milligrams IV lorazepam, Dr. Faust.” So, “thank you" is my way of saying “this is me confirming information, not adding new information.” (There’s a theater version of this. The stage manager says “Five minutes until curtain,” to which an actor may respond, “Thank you, five!”)
Next, I intentionally alter the way each piece of information gets conveyed on my end. “2 milligrams” becomes “2 migs” (“migs” is an abbreviation for milligrams). That way, if anyone misheard the nurse say milligrams, and they then hear me say “migs,” the error is more likely to be noticed. I also turn “loraz’”—which is a perfectly acceptable shortcut for lorazepam—into “lorazepam.” If the nurse says one, I say the other. If they use a trade name (Ativan), I might use the generic (lorazepam). You get the point. Lastly, I say “intravenous,” instead of IV, to distinguish that from an injection into a muscle (which would be an “IM,” or intramuscular route), and which might require a different dose.
The point is, I conspicuously change the wording just a tad when I’m confirming information, as a way of verifying the information with a kind of redundancy that might reveal an otherwise subtle miscommunication.
Another example that I don’t use—but maybe should—is the use of “tree” instead of “three.” In aviation comms, 23,000 feet might be pronounced as twenty-tree thousand feet, because “three” is somehow misheard or mistaken for other words with some frequency. I guess I’m a little self-conscious about going “full aviator” on my colleagues. Then again, we are not on the radio with static and other noise, so maybe “three” is good enough for the ER.
And speaking of 23,000 feet, you may have noticed another practice related to repeating numbers during closed-loop communication. In my “good example” of the pilot and co-pilot closing the communication loops, I had each of them say “23,000 feet.” But even better would be if one had said “twenty-three thousand” and the other responded with “two-three thousand.” Expanding the numbers out like this can be a safety net that prevents a mishap.
Props to the pilots.
The culture of safety in aviation is no accident; it’s a result of a long-standing commitment to standards and procedures that have stood the test of time. Just as important, though? The industry is always learning, updating its training and manuals after things go wrong—or even if they almost do.
The Maui near-miss incident reminded me of the importance of good closed-loop communication. I’ll take back to the hospital with me later this month.
Do you have examples of miscommunications that caused a major problem or almost did? Share them in the comments!
This was a good informative explanation of communication protocol. Thanks.
Good to game this out I agree. Much to learn from miscommunications.
Unfortunately I also see another peril here, which is a necessary part of our jobs as physicians - delegation of tasks. Every time we seek help and delegate to medical assistants, nurses, and other support staff, there is a chance someone drops the baton, or worse, is not paying attention and stops running completely. The copilot in your example really dropped the delegated task (you would think he/she would know 5 degrees might be a bad call?)
A nightmare story from a colleague here in Philly was sensationalized by The Inquirer recently. I almost cancelled my subscription. Basically, an Infertility doctor was handed a syringe full of trichloroacetic acid instead of saline to inject. This was drawn up by the medical assistant. An absolute tragedy for the injured patient, and as a physician I can only imagine the horror, shame, and guilt felt by the physician. Instead of recognizing a double tragedy, primarily for the injured patient but also the doc, the Inquirer vilified the doc, and the malpractice lawyers did much the same en route to what will most certainly be a big payout.
We can't do it all as physicians. But when delegation creates mistakes, it makes us want to take this whole enterprise on our own shoulders... which we can't and shouldn't do.