

Lowering blood pressure in ambulances didn't improve stroke outcomes.
Lowering blood pressure in ambulances didn't improve stroke outcomes.
Your "Five on Friday" lead story for May 24, 2024...


We are back with “Five on Friday", the feature where Inside Medicine behaves like an actual medical/health/science newsletter. Below are the top-of-mind things that I’m thinking about right now.
Also, please vote in the poll at the end!
If you value this feature—and Inside Medicine in general…
Here we go…

Item 1: Lowering blood pressure in possible stroke patients sooner? Nope.
May is Stroke Awareness Month. First off, if you’re worried someone is having a stroke, do not do any simple testing, as some well-meaning healthcare messaging efforts often advise. That delays things. Just call 911.
Meanwhile, a new study in the New England Journal of Medicine (NEJM) found that efforts to lower blood pressure in patients with suspected strokes while they were being transported to the ER did not improve outcomes. This is important for a few reasons. First, we should not spend money on things that do not help. Second, it implies that some of our hospital-based treatments don’t work as well as we think. For example, patients with excessively high blood pressure are not supposed to get clot-busting drugs used to treat strokes. If lowering blood pressure meant that more patients arrived to the ER in a condition that allowed them to get clot-busting drugs, it would follow that outcomes should have been better. But that assumes that clot-busting drugs for stroke work as well as advertised. This new study seems to throw shade at that concept, but I noticed that the authors did not choose to mention this. (They clearly would have if the results had come out differently, as I assume this was the point of the study.)
Item 2: Marijuana legalization associated with more geriatric ER visits.
Behind many efforts to legalize marijuana was a belief that its active ingredient (THC) is not all that harmful. I’ve never subscribed to that belief. Like all substances, a risk-benefit analysis can be performed.
Whatever medical benefits there may be, legalization of recreational marijuana (2018) was associated with a doubling of geriatric ER visits for THC-related toxicity in Canada and a tripling with the legalization of edible forms of cannabis (2020), according to a new study in JAMA Internal Medicine. Poisoning events were more likely in males, and, somewhat surprisingly, higher among 65-74 year-olds than people ages ≥75.
Previous research has shown that marijuana legalization may have harmful effects at the population level with respect to auto fatalities.
Two comments: 1. The dose makes the poison; 2. Recreational substance use should always prioritize safety.
Item 3. Specialists helped asthma and emphysema patients.
A new study in NEJM studied whether patients with newly diagnosed asthma or emphysema (a.k.a., chronic obstructive pulmonary disease, or COPD) benefited from seeing a specialist. First, researchers identified a cohort of patients with undiagnosed asthma or COPD. Then, these patients were randomized either to see a pulmonologist or their primary care doctor.
The patients who were randomized to see a pulmonologist went on to have fewer emergency visits (either to the clinic or the hospital). This implies that the specialists were able to intervene in a way that decreased flare ups. That said, the absolute differences were small and a cost-effectiveness analysis might not work out. What we don’t know is whether a refresher on modern asthma and COPD management among the primary care docs would have achieved the same benefits. The analysis would hinge on how much more speciality care costs and whether the medications that specialists prescribe (that ostensibly decreased the need for emergency care) were a lot more (or just a little) more expensive than what primary care docs recommended.
Item 4: Osteoporosis drugs reduce some but increase other fractures.
Patients with osteoporosis are often prescribed drugs called bisphosponates, including one called Fosamax. These drugs decrease the risk of fractures overall, but they also may increase the risk of certain really nasty ones. “Fosamax fractures” have been a known entity for a long time, it turns out. (I noticed these during residency, but found it is not often discussed by physicians, nor are the risks typically known to patients who take these medications). An essay in the Journal of the American Medical Association lays the story out well. A group of Fosamax fracture patients sued Merck over this, but the cases remain unresolved, largely due to the complexities of how black box warnings come about, and how the FDA adjudicates issues like this.
A larger issue is that not all drugs that doctors think patients needed to take turn out to be necessary. For example, a recent study appearing in the British Medical Journal found that systematically de-prescribing medications for acid reflux (proton pump inhibitors such as Prilosec and Nexium) had no negative effects on patients, and, naturally, doing so saved money.
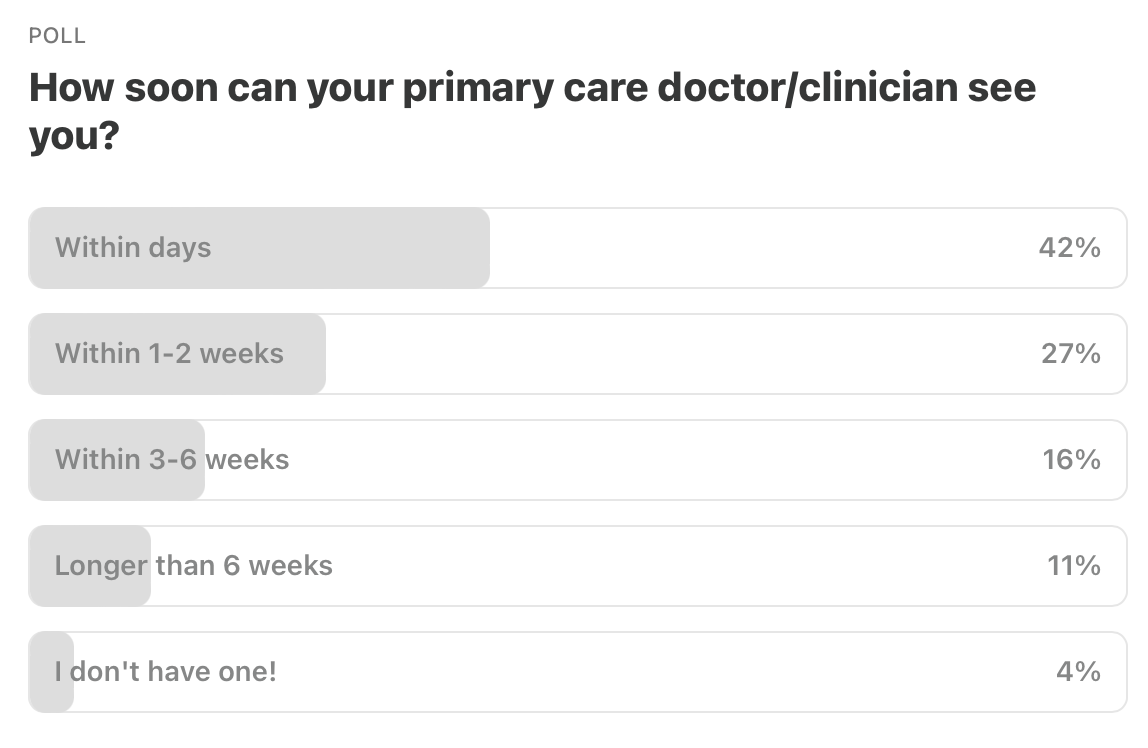
Item 5. Poll of the Week.
Here are the results from last week’s poll.
Item 5a. Poll of the Week for this week!
A recent study found that certain patients of women physicians have better outcomes compared to physicians who are men. Recognizing that there is a lot of nuance here…
I’d love to hear your reasoning and imagine some of you will be willing to share your views. So this is one where I expect the Comments section to be lively! Thanks for chiming in.
That’s it. Your “Friday Five!”
Feedback! Do you like the “Five on Friday” format? Have any ideas for next week’s Poll of the Week? Any great articles you read elsewhere that you want to share with the Inside Medicine community? Other musings or thoughts?
Please contribute to the Comments!
I've had both primary care and specialist providers of both genders; ditto with physical therapists and nurses. I've had good to excellent relationships and care from most, regardless of gender; the few I've moved quickly to change from have been equally divided as to gender - people who just didn't listen to me, or made clear that if I raised questions, they didn't want to waste time with me. One anecdotal observation: both my wife and I have (now and formerly) primary care provided by nurse practitioners (all women; in practices overseen by MDs/DOs), and have found them on the whole more willing to spend time and pursue options than the primary-care MDs we've had.
The only healthcare provider that I prefer to be a woman is my gynecologist. This is not because of modesty, but rather because I think another woman is more likely to truly understand some of the issues unique to women's health in that arena.